Everyone has a story to tell, and here we share and celebrate those who chose care as their life's work.
These are their words, their work and we're grateful to share them.
Elizabeth and Dennis handed their billing to Carepatron and grew My Therapeutic Concepts from five clients to seventy in two months, without losing their evenings.
Handling patients who come into the emergency room can be quite a fright, not just for the patient's loved ones or friends, but also for the healthcare providers assessing them, no matter how composed they are. All the more if they're brought in because of a traumatic brain injury or an accident that has rendered them unconscious or barely conscious.
If you're handling patients who are unconscious because of accidents or a brain injury, it's important to be prepared and immediately assess their levels of consciousness. Having the Glasgow Coma Scale at the ready is beneficial for timely and efficient treatment, enabling the patient(s) to undergo necessary stabilization and recovery. Read on to learn more about this important staple tool.
## **What are the levels of consciousness?**
Before discussing the Glasgow Coma Scale (GCS), it’s important to understand the levels of consciousness it aims to measure. Assessing a patient provides critical insight into brain function and neurological status, guiding decisions about care and intervention. Clinicians often use standardized terminology to describe these states of alertness or unresponsiveness, which range from full wakefulness to deep coma. The following descriptions are based on Bickley and Szilagyi (2004) and Hinkle and Cheever (1996):
- An alert patient opens their eyes spontaneously, makes purposeful movements, looks at you when spoken to, and responds appropriately to stimuli.
- A lethargic patient is somewhat drowsy but can still open their eyes and respond to loud verbal cues. They can answer questions and maintain eye contact, although they may easily drift back to sleep.
- In obtundation, the patient shows signs of confusion and fluctuating awareness. They can open their eyes and respond to touch or voice, but their responses are slow and often lack clarity.
- A stuporous patient is unresponsive, mainly only awakening to painful stimuli. Verbal responses are minimal or absent, and once the stimulus stops, they usually lapse back into unresponsiveness.
- A comatose patient cannot be aroused at all—their eyes remain closed, and they show no purposeful response to verbal or physical stimuli. Non-purposeful movements may occur with painful stimulation, and some may exhibit brainstem reflexes, though these are not always present.
Understanding these levels of consciousness provides a foundation for interpreting the Glasgow Coma Scale, which offers a more objective, numerical approach to assessing neurological status.
## **What is the Glasgow Coma Scale (GCS)?**
The Glasgow Coma Scale is a widely used clinical scale that assesses the level of consciousness and neurological function in patients with acute brain injury or impaired consciousness. Developed by Sir Graham Teasdale and Bryan Jennett at the University of Glasgow in 1974, the GCS provides a structured approach to evaluating and communicating a patient's condition (Teasdale et al., 2014).
This practical scale's structured approach is widely used in various clinical practice settings, including the emergency department, intensive care units, research in neurological sciences, and trauma centers. It is particularly useful in the initial assessment and management of trauma patients.
### **Primary uses of the GCS**
1. In cases of mild traumatic brain injury, such as a concussion or moderate injury, the GCS helps determine the severity of the injury and guides appropriate management and monitoring.
2. The GCS is essential in the assessment and early management of moderate to severe traumatic brain injuries, which may result from events like a car accident, a fall, or in cases of severe injuries. It aids in triaging patients, predicting outcomes, and guiding treatment decisions.
3. The scale can be used to assess the level of consciousness in intubated patients, particularly when verbal responses are impossible, such as in patients in deep coma. In such cases, alternative scoring methods like the GCS-P score (pupil reactivity) or the simplified motor score may be employed.
4. It's also recommended for evaluating patients with acute brain damage or impaired consciousness due to various causes, such as stroke, intracranial hemorrhage, blunt head trauma, or even severe brain damage. It helps assess the patient's consciousness level and neurological status, guiding further diagnostic tests and interventions.
5. In the context of advanced trauma life support, the GCS is a crucial component of the primary survey. It provides a structured approach to assessing the patient's level of consciousness and neurological function, which can inform the management of life-threatening injuries.
6. For assessing younger children, a modified version called the Pediatric Glasgow Coma Scale (PGCS) may be used, as it accounts for developmental differences in verbal and motor responses.
### **Components of the Glasgow Coma Scale**
The Glasgow Coma Scale assessment process involves testing the eye-opening, verbal, and motor responses. Each component is scored independently, and the sum of these scores determines the overall GCS score (Jain & Iverson, 2023).
- **Eye-opening response**: The eye-opening response is scored on a scale of 1 to 4, with 4 being the best eye-opening response (spontaneous eye-opening) and 1 being the worst (no eye-opening).
- **Verbal response**: The verbal score ranges from 1 to 5, with no verbal response (1) and oriented and conversing normally (5) being the best verbal response. It assesses the patient's ability to respond verbally to questions or commands.
- **Motor response**: This is scored on a scale of 1 to 6, with 6 being the best motor response (obeying commands) and 1 being the worst response (no motor response). It evaluates the patient's ability to follow verbal commands and move their extremities.
## **How to use this Glasgow Coma Scale template**
Carepatron's Glasgow Coma Scale template is a great way to securely and accurately record your patient's GCS results. Not only that, but it can also be used digitally. If you're in a rush to assess your patient, which is likely, you can use our PDF template. This allows you to easily tick your ratings based on their responses (or the lack thereof).
Here's a step-by-step guide on how to use this tool:
### **Step 1: Introduce the test**
Before administering the Glasgow Coma Scale, it's essential to introduce the test to the patient (if they are conscious) or their family members. Explain that the GCS is a standardized assessment tool used to evaluate the patient's level of consciousness and neurological function in case of a head injury. Reassure them that the process is noninvasive and will involve observing their responses to various stimuli.
### **Step 2: Assess eye-opening response**
Begin by evaluating the patient's eye response. Observe if they open their eyes spontaneously (score 4), in response to verbal stimuli (score 3), in response to painful stimuli (score 2), or if they do not open their eyes at all (score 1).
### **Step 3: Evaluate verbal response**
Next, assess the patient's verbal performance. Determine if they are oriented and conversing normally (score 5), confused or using inappropriate words (score 4), uttering incomprehensible sounds (score 3), making no verbal response (score 2), or completely unresponsive (score 1).
### **Step 4: Examine motor response**
The motor scale evaluates the patient's motor response by observing their ability to follow commands. The motor score is 6 if they obey commands, 5 if they localize to painful stimuli, 4 if they withdraw from painful stimuli, 3 for abnormal flexion (decorticate posturing), 2 for abnormal extension (decerebrate posturing), and 1 for no motor response.
### **Step 5: Calculate the Glasgow Coma Scale score and interpret**
Add the total score for eye-opening, verbal response, and motor response to obtain the total GCS score. The maximum GCS score is 15, indicating a fully awake and responsive patient, while the minimum score is 3, indicating a deeply comatose state. Remember that the GCS is a screening tool and should be used in conjunction with other clinical assessments and diagnostic tests.
## **Scoring and interpretation**
When using the Glasgow Coma Scale, it's essential to understand how to score and interpret the results correctly. The GCS provides a standardized and structured approach to assessing a patient's level of consciousness and neurological function, particularly in cases of traumatic brain injury or acute brain damage.
These individual components are scored independently on a scale, and the sum of these scores determines the overall Glasgow coma score.
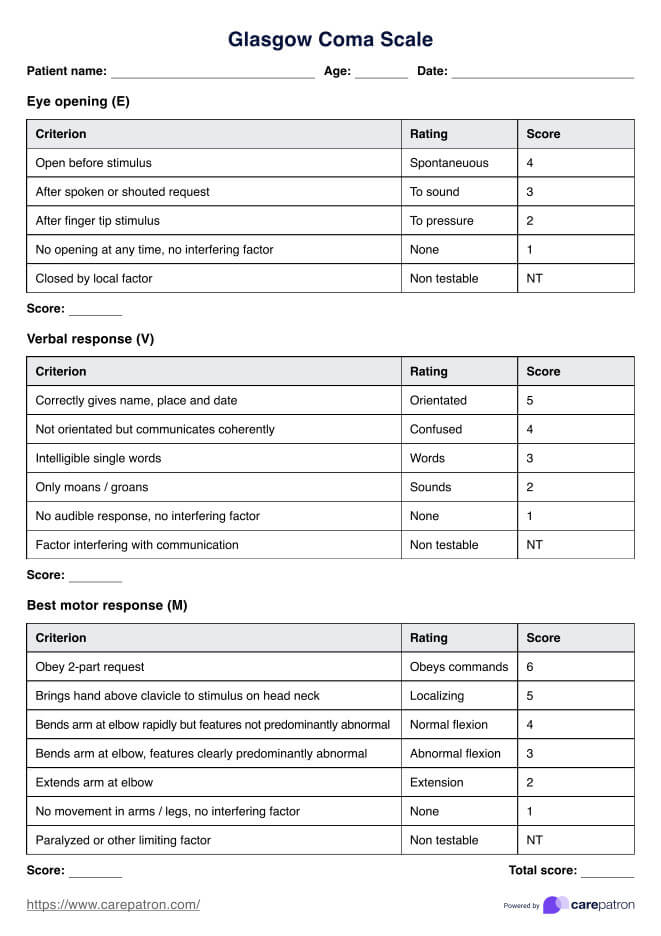
The following scores are given for the eye-opening response:
- **Score 4**: Spontaneous eye opening
- **Score 3**: Eye opening in response to verbal stimuli
- **Score 2**: Eye opening in response to painful stimuli or pressure
- **Score 1**: No eye opening
- **NT**: Non-testable
For the verbal response, the following observations are to be noted:
- **Score 5**: Oriented and conversing normally
- **Score 4**: Confused
- **Score 3**: Uttering intelligible single words
- **Score 2**: Only moans and groans
- **Score 1**: No verbal response
- **NT**: Non-testable
The following scores are then given for motor response:
- **Score 6**: Obeying commands
- **Score 5**: Localizing to painful stimuli
- **Score 4**: Normal flexion
- **Score 3**: Abnormal flexion
- **Score 2**: Extension
- **Score 1**: None
- **NT**: Non-testable
The total coma score is the sum of the individual component scores, ranging from a maximum of 15 (fully awake and responsive) to a minimum of 3 (deeply comatose state). The GCS score is commonly interpreted as follows:
- **13-15**: Mild brain injury
- **9-12**: Moderate brain injury
- **3-8**: Severe brain injury
It's important to note that the GCS is a screening tool and should be used in conjunction with other clinical assessments and diagnostic tests. It provides a reliable and consistent method for assessing and communicating a patient's level of consciousness and neurological function, aiding in triage, treatment decisions, and monitoring of their condition over time.
## **Next steps after using the Glasgow Coma Scale**
What you need to do for the patient will depend on how severe their traumatic brain injury is, or if they're unconscious or not (Mayo Clinic, 2021).
For mild injuries, the patient simply needs to rest and take over-the-counter pain medicine. Even if the injury is mild, it would be best to monitor the patient or have one of their loved ones monitor them, just in case other traumatic brain injury symptoms emerge over time.
For those with moderate or severe traumatic brain injuries, it's important to treat them immediately, such as providing anti-seizure medication, coma-inducing drugs, or diuretics. Surgery should be considered only as a last resort or when it is the only option initially.
If the traumatic brain injury has lasting effects on the patient, they will need rehabilitation. What kind of rehabilitation they need will depend on what effects they are grappling with. Some professionals who can help with rehabilitation include physical therapists, occupational therapists, speech and language therapists, and neuropsychologists. Please make any referrals to the relevant specialists to help the patient recover.
## **References**
Bickley, L. S., & Szilagyi, P. G. M. (2004). Bates’ guide to physical examination and history taking. http://bibliocissslanaudiere.visard.ca/Record.htm?Record=19176476124919946589
Hinkle, J. L., & Cheever, K. H. (1996b). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. http://ci.nii.ac.jp/ncid/BB15317023
Jain, S., & Iverson, L. M. (2023, June 12). Glasgow coma scale. National Library of Medicine; StatPearls Publishing.
Mayo Clinic. (2021, February 4). Traumatic brain injury - Diagnosis and treatment - Mayo Clinic. Mayoclinic.org. https://www.mayoclinic.org/diseases-conditions/traumatic-brain-injury/diagnosis-treatment/drc-20378561
Teasdale, G., Maas, A., Lecky, F., Manley, G., Stocchetti, N., & Murray, G. (2014). The Glasgow coma scale at 40 years: Standing the test of time. The Lancet Neurology, 13(8), 844–854. https://doi.org/10.1016/s1474-4422(14)70120-6
Commonly asked questions
The Glasgow Coma Scale (GCS) is a clinical tool used to assess a patient’s level of consciousness after a head injury. It evaluates three responses—eye opening, verbal response, and motor response—each scored separately and summed for a total score between 3 and 15. Higher scores indicate better neurological function, while lower scores suggest more severe impairment.
A GCS score of 3 is the lowest possible score, reflecting no eye opening, no verbal response, and no motor response. However, a GCS of 3 does not automatically mean brain death; it only indicates deep coma or unresponsiveness. Brain death requires additional confirmatory tests, such as absent brainstem reflexes and lack of spontaneous breathing.
A GCS score of 14 is considered near normal, typically indicating mild confusion or disorientation. It may occur after minor head trauma or transient medical conditions, but generally reflects preserved neurological function. Continuous monitoring is recommended to ensure the score does not decline, signaling worsening brain injury.