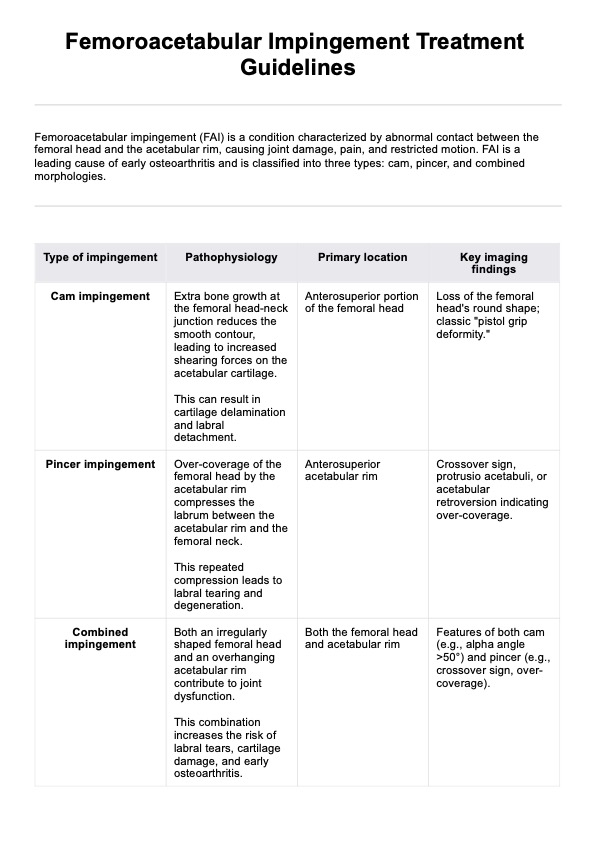
A femoral acetabular impingement occurs when an abnormally shaped femoral head or hip socket disrupts the smooth movement of the ball-and-socket joint. This can damage the labrum and articular cartilage, resulting in hip or groin pain and reduced range of motion. Diagnosis typically involves a combination of a detailed medical history, physical exams such as the impingement test, and imaging tests like magnetic resonance imaging (MRI) or X-rays to detect bony abnormalities, labral tears, or bone spurs.
Femoroacetabular Impingement Treatment Guidelines
Download our free Femoroacetabular Impingement Treatment Guidelines Handout – a comprehensive resource to educate patients on treatment options.

Use Template
Femoroacetabular Impingement Treatment Guidelines Template
Commonly asked questions
Initial treatment focuses on nonsurgical methods to alleviate pain and improve hip function. Physical therapy is a cornerstone, targeting hip stabilizer muscles and increasing the hip’s range of motion. Activity modification, such as avoiding prolonged sitting or repetitive deep flexion, helps prevent further joint stress. Nonsteroidal anti-inflammatory drugs (NSAIDs) may provide pain relief, especially for labral injuries or inflammation. These measures aim to reduce symptoms while delaying or avoiding surgical procedures.
Surgical treatment is recommended when nonsurgical treatment fails, or pain persists despite initial interventions. Arthroscopic procedures, a minimally invasive option, are commonly used to reshape cam lesions or pincer-type impingement, remove extra bone or bone spurs, and repair labral tears. Open surgery may be necessary for more complex deformities. Surgical procedures are often performed on an outpatient basis, with small incisions minimizing recovery time and scarring.










EHR and practice management software
Get started for free
*No credit card required
Free
$0/usd
Unlimited clients
Telehealth
1GB of storage
Client portal text
Automated billing and online payments