Coracoid Pain Test
Learn about the Coracoid Pain Test for diagnosing adhesive capsulitis (frozen shoulder), including its procedure, interpretation, and management.

Fact Checked by Ericka Pingol.


What is a frozen shoulder?
Frozen shoulder, or adhesive capsulitis, restricts shoulder joint movement, causing stiffness and pain that makes daily tasks challenging. While the exact cause of adhesive capsulitis is unclear, factors like shoulder injuries, post-surgery immobilization, and conditions like diabetes can increase your risk. Symptoms of adhesive capsulitis can develop gradually and may last up to three years.
Hollmann et al. (2015) found that patients with suspected frozen shoulder showed significant improvement in passive abduction under anesthesia, suggesting that loss of motion in the anterior shoulder is not solely due to capsular contraction but also involves muscle guarding or active stiffness.
Common signs include:
- Pain is often worse at night, potentially disrupting sleep.
- Stiffness can significantly limit your ability to move your arm.
- Painful shoulder or an aching or burning sensation within the shoulder joint.
How to diagnose a frozen shoulder?
Diagnosing a frozen shoulder or painful shoulder, often involves visiting a healthcare professional who will conduct a comprehensive physical examination. This evaluation focuses on two key aspects:
- Physical examination: The healthcare professional will assess your range of motion in all directions, particularly internal rotation, a common limitation in a frozen shoulder. They will also check for tenderness in specific areas around your shoulder girdle, including the glenohumeral joint (shoulder joint) itself, the acromioclavicular (AC) joint where the collarbone meets the shoulder blade, and potentially the pectoralis minor muscle located beneath the collarbone. This helps determine the severity of your pain and how much your movement is restricted.
- Imaging tests: While not always necessary, X-rays or MRI scans may be used to rule out other potential causes of your pain, such as rotator cuff tears or arthritis. These imaging studies provide detailed pictures of your shoulder's bones and soft tissues, aiding in a definitive diagnosis.
Coracoid Pain Test Template
Coracoid Pain Test Example
What is the Coracoid Pain Test?
The Coracoid Pain Test is a clinical method used to diagnose shoulder adhesive capsulitis only, commonly known as frozen shoulder. This test checks whether pressure applied to the coracoid process area of the shoulder blade causes pain, which may indicate the presence of this condition.
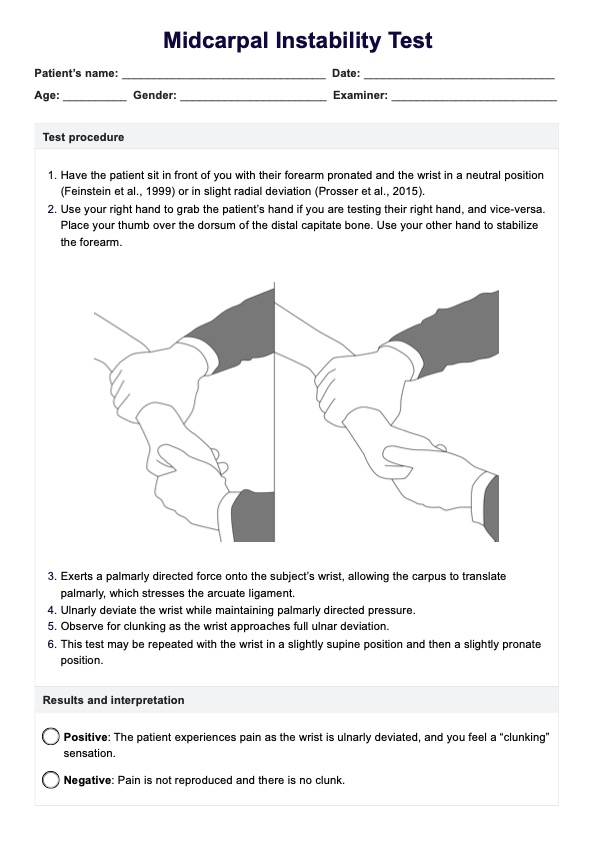
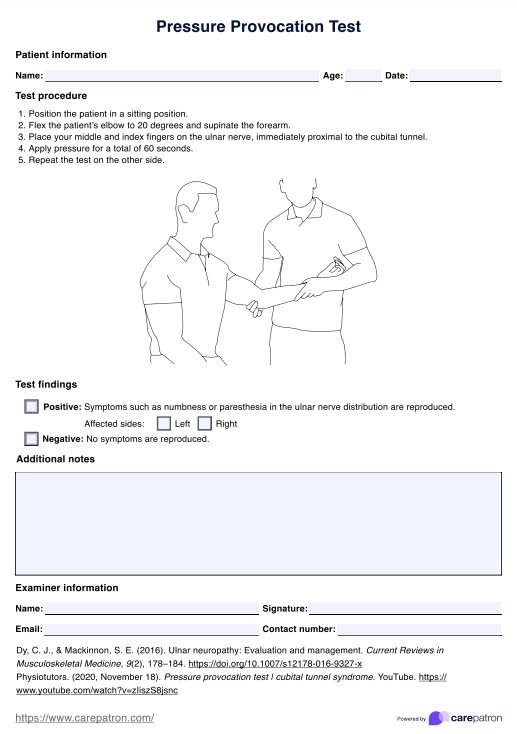
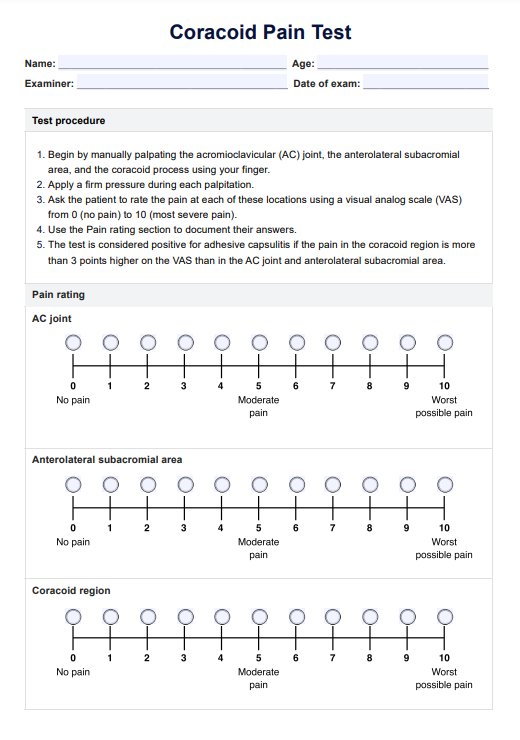
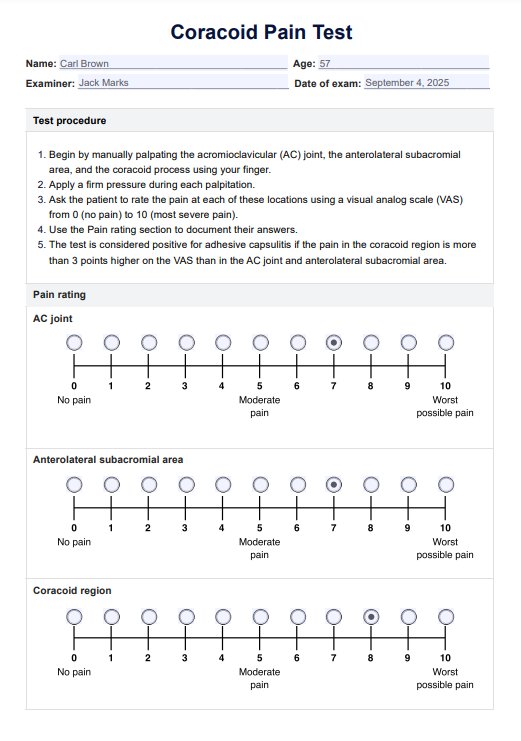
How to perform the test:
- Begin by manually palpating the AC joint, the anterolateral subacromial area, and the coracoid process using your finger.
- Ask the patient to rate the pain at each of these locations using a visual analog scale (VAS) from 0 (no pain) to 10 (most severe pain).
- The test is considered positive for adhesive capsulitis if the pain in the coracoid region is more than 3 points higher on the VAS than in the AC joint and anterolateral subacromial area.
Our Coracoid Pain Test template is designed for use during the actual assessment to ensure accurate clinical documentation during the Coracoid Pain Test. This template helps systematically record the palpation points and the patient's pain ratings, ensuring that all relevant data is captured for proper diagnosis and treatment planning.
Results and interpretation of the Coracoid Pain Test
The Coracoid Pain Test results are determined by the pain scores you report while palpating three specific frozen anterior shoulder pain side areas. A positive test indicates a higher likelihood of a frozen anterior shoulder pain but is not a definitive diagnosis. Here's how the coracoid region interpretation works:
As mentioned, the test is considered positive if the patient experience significantly more pain (at least 3 points higher in the VAS) when pressure is applied to the coracoid process compared to the AC joint capsule and anterolateral subacromial area. This increased tenderness in the coracoid process is often seen in frozen shoulder patients.
If there is minimal or no difference in pain scores between the three areas, the test is considered negative for clinical signs of a frozen shoulder. Pain may still be present, but it is unlikely to originate from the coracoid process or indicate a frozen shoulder.
Benefits of using our template
Our downloadable Coracoid Pain Test template offers multiple advantages for healthcare professionals and patients alike:
- Enhanced efficiency: The template provides a pre-formatted structure for recording test results, saving valuable time during physical examination, and documentation. This allows healthcare professionals to focus more on patient interaction and analysis.
- Improved consistency: The standardized format ensures a consistent approach to administering and recording the Coracoid Pain Test across different healthcare providers. This consistency promotes reliable data collection and facilitates better comparison of results over time.
- Clear communication: The template includes designated sections for recording patient information, pain scores, and any observations made during the test. This clear presentation enhances communication and collaboration between healthcare professionals involved in the patient’s care.
- Educated patients: The template can be customized to include a patient education section with illustrations new clinical sign or explanations of the test procedure. This improves patient understanding of the diagnosis and encourages better engagement in their treatment plan.
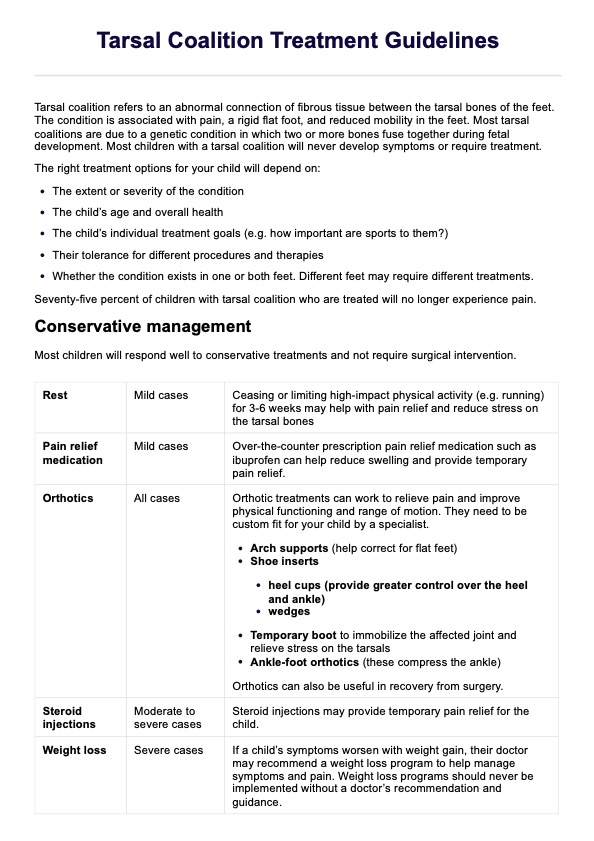
Treatment of shoulder adhesive capsulitis
Treatment for shoulder adhesive capsulitis, or frozen shoulder, aims to relieve pain and restore movement in the shoulder joint. The primary approach is physical therapy, which includes a tailored exercise program to stretch and strengthen the shoulder capsule, rotator cuff, and surrounding muscles. This therapy helps improve flexibility and range of motion, addressing issues like a stiff shoulder and conditions affecting the rotator cuff interval.
Pain management typically involves nonsteroidal anti-inflammatory drugs (NSAIDs) or prescription pain relievers to reduce pain and inflammation. These treatments are especially beneficial for conditions like coracoid impingement, subcoracoid impingement, and irritation of the biceps tendon. Corticosteroid injections may be administered to provide targeted relief by reducing inflammation and potentially enhancing the effectiveness of physical therapy. In cases where conservative treatments are ineffective, surgery might be necessary.
Surgical options may include manipulating the shoulder joint under anesthesia to loosen scar tissue or performing arthroscopic surgery to remove scar tissue, which can help alleviate issues related to the process, rotator cuff tear, and the acromioclavicular joint, while improving overall shoulder function.
Reference
Hollmann, M., Wieczorek, V., Berger, S., & Hintermeister, R. (2015). Range of motion in anterior shoulder instability. Physiotherapy, 101, e585-e586.
Commonly asked questions
A Coracoid Pain Test is used to diagnose frozen shoulder syndrome, also known as adhesive capsulitis. This test helps determine if the pain is caused by inflammation in the coracoid process of the scapula (shoulder blade), which can be a contributing factor to frozen shoulder syndrome.
Coracoid process pain is typically felt near the front of the shoulder, just below the collarbone. This area is often sensitive to touch and can cause a deep, aching pain that may radiate down the arm.
There are several ways to fix a coracoid impingement, depending on the severity of the condition. These may include physical therapy exercises to strengthen the surrounding muscles and improve range of motion, anti-inflammatory medication or corticosteroid injections to reduce pain and inflammation, and in more severe cases, surgery to remove any bony growths or repair damaged tissues.
Related Templates

Popular Templates