Neer's Classification
Discover Neer's Classification for proximal humerus and distal clavicle fractures, including types, symptoms, and treatments. A comprehensive guide for healthcare professionals and students.

Fact Checked by Ericka Pingol.


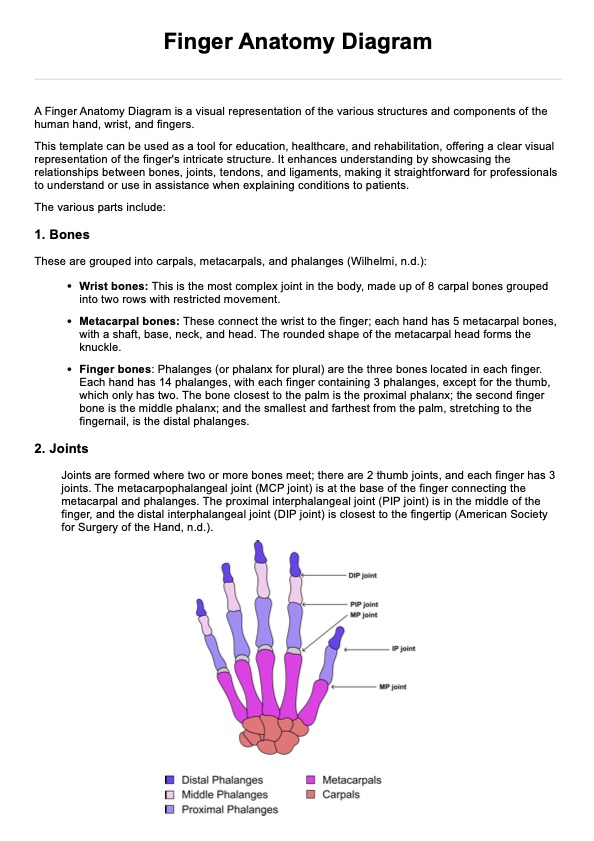
What is a proximal humerus fracture?
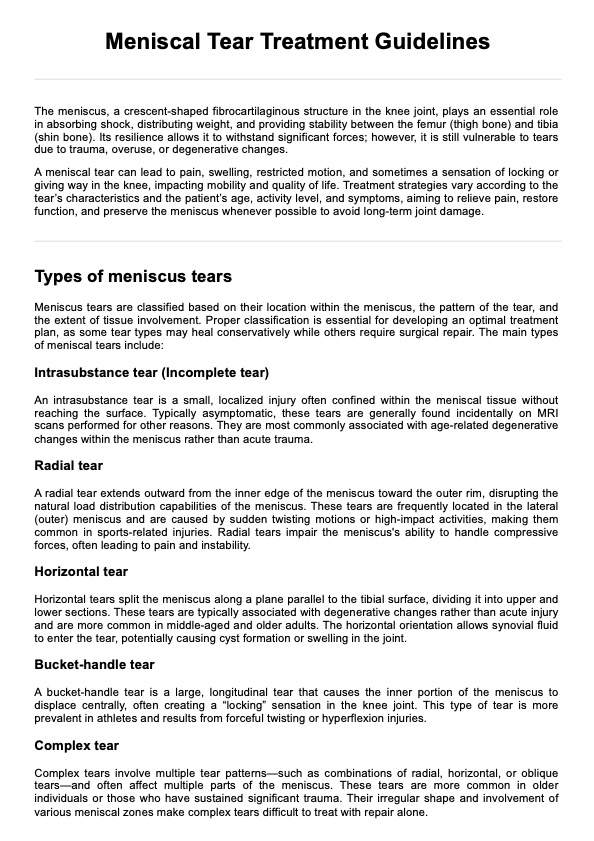
A proximal humerus fracture refers to a break in the upper part of the arm bone (humerus) near the shoulder. These fractures are relatively common, especially among older adults with osteoporosis. The proximal humerus fracture can result from a direct blow to the shoulder, a fall, or a motor vehicle accident. It is more prevalent in women due to their higher risk of osteoporosis, but it can affect individuals of all ages, particularly those involved in high-impact sports or activities.
Symptoms
The symptoms of displaced proximal humeral fractures can vary in severity but typically include:
- Pain: Severe pain in the shoulder or upper arm.
- Swelling and bruising: Visible swelling and bruising around the shoulder.
- Limited mobility: Difficulty moving the shoulder or arm.
- Deformity: Visible deformity or bump at the fracture site.
- Numbness or tingling: Possible numbness or tingling in the arm or hand if nerves are affected.
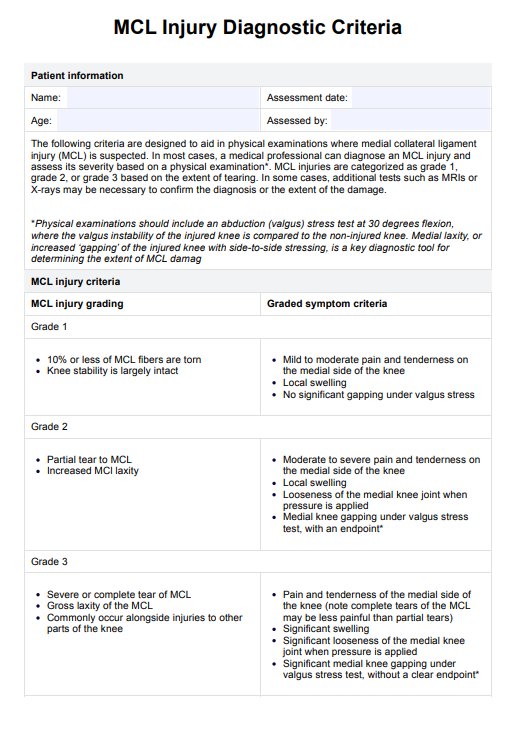
How to classify proximal humerus fractures
Classifying proximal humerus fractures involves assessing the fracture's complexity, displacement, and involvement of different parts of the bone. The most commonly used classification systems are the Neer Classification and the Arbeitsgemeinschaft für Osteosynthesefragen-Orthopaedic Trauma Association (AO/OTA) classification. Medical imaging, particularly X-rays and CT scans, is essential in accurately diagnosing and classifying these fractures. The classification helps determine the appropriate treatment plan, ranging from conservative management to surgical intervention.
Neer's Classification Template
Neer's Classification Example
What is the Neer Classification system?
The Neer Classification system is a widely used method for categorizing proximal humerus fractures. Developed by Dr. Charles Neer in the 1970s and published in The Journal of Bone & Joint Surgery (J Bone Joint Surg), this system helps healthcare professionals assess the severity and complexity of adult fractures to guide treatment decisions. The classification system is based on the anatomical parts of the proximal humerus and the degree of displacement of the fractured segments. It is particularly valuable for identifying the need for surgical intervention versus conservative management.
Neer's original classification focused on proximal humeral fractures, adjustments have been made to it to consider distal clavicle fracture and displacement, making it a significant tool in orthopedic practice for assessing and managing these injuries. However, this guide and template covers the original classification.
How does it describe a fracture?
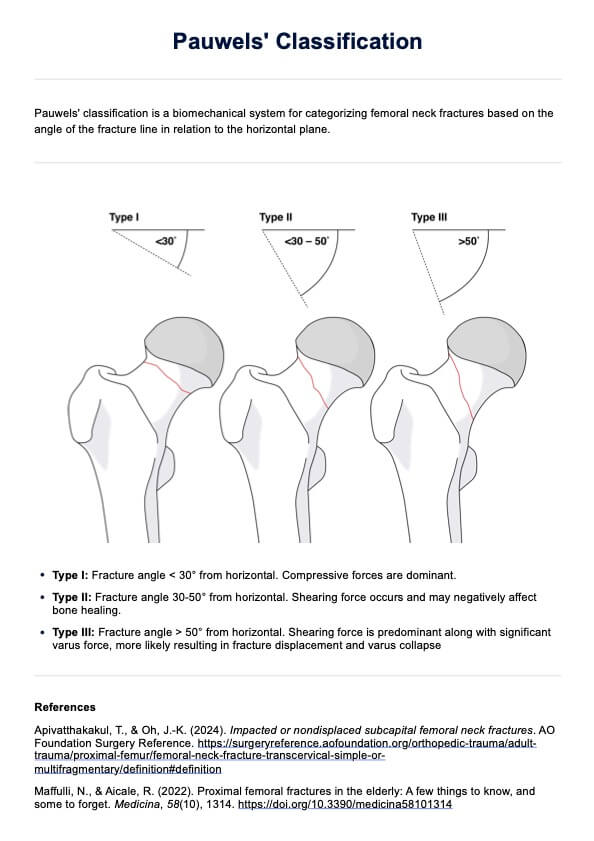
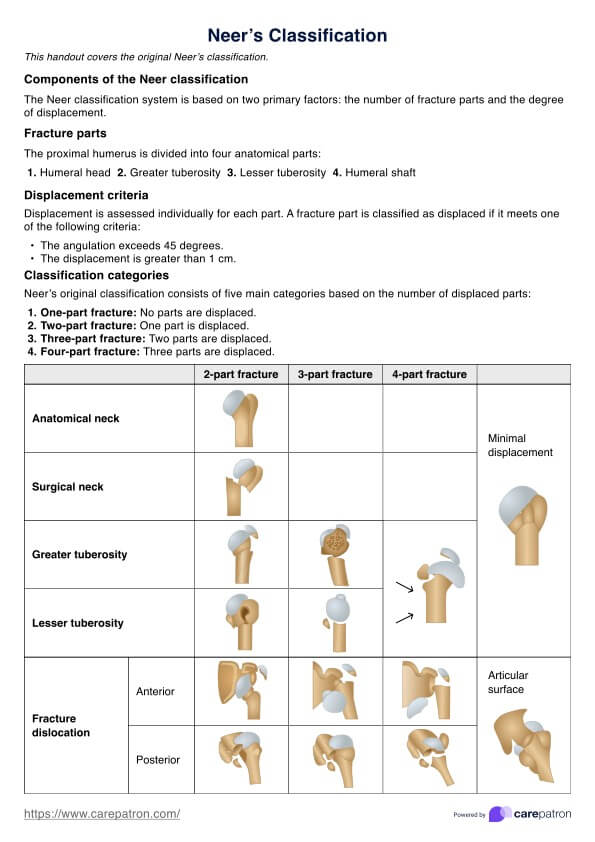
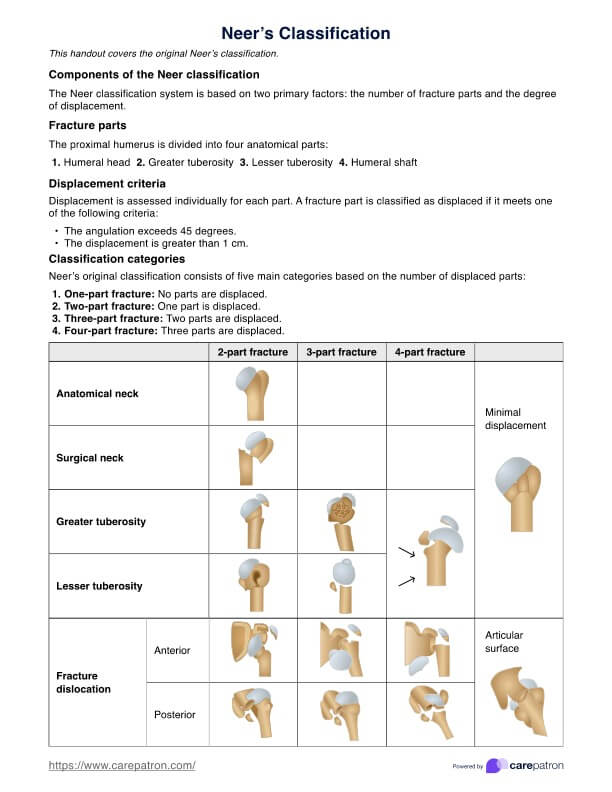
The Neer Classification system describes a fracture based on two primary factors: the number of displaced parts and the degree of displacement. The proximal humerus is divided into four anatomical parts: the humeral head, greater tuberosity, lesser tuberosity, and surgical neck. The involvement of the articular surface also plays a part in determining the type and severity of each fracture.
A fracture part is considered displaced if it meets one of the following criteria:
- The angulation exceeds 45 degrees.
- The displacement (or gap in the fracture lines) is greater than 1 cm.
Types of fractures in the Neer's Classification
The original Neer's Classification consists of five main categories, with varying fracture patterns:
- One-part fracture: No parts are displaced.
- Two-part fracture: One part is displaced.
- Three-part fracture: Two parts are displaced.
- Four-part fracture: Three parts are displaced.
For a detailed diagram displaying a fracture pattern for each category, look at our template.
How does our Neer's Classification template work?
Our Neer's Classification template is designed to provide healthcare professionals with a straightforward and efficient tool for diagnosing and categorizing proximal humerus fractures.
Step 1: Download the template
Begin by downloading or accessing the Neer's Classification template from the provided link on this page or via the Carepatron app.
Step 2: Familiarize yourself with the handout
Review the template thoroughly to understand its structure and the information it contains. Familiarizing yourself with the classification categories and criteria will ensure accurate use during patient assessments.
Step 3: Use the template for diagnosing proximal humerus fractures
Follow the procedures outlined in the template to classify the proximal humerus fracture. The template provides clear definitions and criteria for each type of fracture, making it easy to identify the specific classification based on the patient's X-ray or clinical examination findings.
Step 4: Document findings and additional notes
Use the designated field in the template to record your findings, including the fracture classification, displacement details, and any notes. This documentation will assist in tracking the patient's progress and informing subsequent treatment decisions.
Treatments for displaced proximal humeral fractures
When treating proximal humeral fractures, the approach depends on the severity of the fracture, the patient's overall health, and their functional requirements. Here are some common treatment options:
- Non-surgical management: This includes immobilization using a sling or brace, allowing the bone to heal naturally. This is the first option for minimally displaced fractures.
- Pain management: Medications such as acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs) can help manage pain and inflammation during the healing process.
- Physical therapy: After immobilization, physical therapy is crucial for regaining range of motion, strength, and function in the affected shoulder. Exercises may start with gentle range-of-motion activities and gradually progress to strengthening exercises.
Surgical intervention
For more severe fractures, surgical options are often necessary. These can include:
- Open reduction and internal fixation (ORIF): This procedure involves realigning the broken bone fragments and securing them with metal plates, screws, or pins. ORIF is typically used for fractures where the bone pieces are displaced and need precise alignment to heal correctly.
- Hemiarthroplasty: This surgical option involves replacing the head of the humerus with a prosthetic implant. It is generally considered when the humeral head is severely damaged or fragmented.
- Total shoulder arthroplasty: Also known as shoulder replacement surgery, this involves replacing both the head of the humerus and the socket of the shoulder blade with prosthetic components. This option is typically reserved for patients with extensive joint damage or concurrent arthritis.
- Reverse total shoulder arthroplasty: This specialized form of shoulder replacement is used when there is significant damage to the rotator cuff. It reverses the normal ball-and-socket configuration of the shoulder joint, providing more stability and function for patients with severe rotator cuff injuries and fractures.
Proximal humerus fractures treated surgically also require significant post-operative care as they come with a risk of avascular necrosis.
Reference
Neer, C. S. (1970). Displaced proximal humeral fractures. I. Classification and evaluation. Journal of Bone and Joint Surgery, 52(6), 1077-1089.
Commonly asked questions
Neer's classification categorizes proximal humeral fractures based on the number and displacement of fracture parts, including one-part, two-part, three-part, and four-part fractures.
The classifications include one-part (non-displaced), two-part, three-part, and four-part fractures. The modified Neer classification for distal clavicle fractures includes Type I (lateral to CC ligaments), Type IIa (medial to CC ligaments with displacement), Type IIb (between CC ligaments with torn conoid ligaments), Type III (intra-articular), Type IV (Salter-Harris type I), and Type V (comminuted with medial displacement).
The four parts are the humeral head, greater tuberosity, lesser tuberosity, and surgical neck.
Related Templates

Popular Templates