


What is a Medical History Form?
Patient care can pose challenges, particularly during transitions between healthcare providers or when patients are referred to a new practitioner as part of their treatment journey.
While patients may willingly offer relevant details about their medical history, the process becomes significantly smoother and more effective when accompanied by a comprehensive Medical History Form from a prior healthcare provider. Documenting and reviewing the patient's health journey, family medical history, past medical interventions, surgeries, tests, treatments, and psychiatric health issues is crucial to determining the patient's care requirements and risk factors.
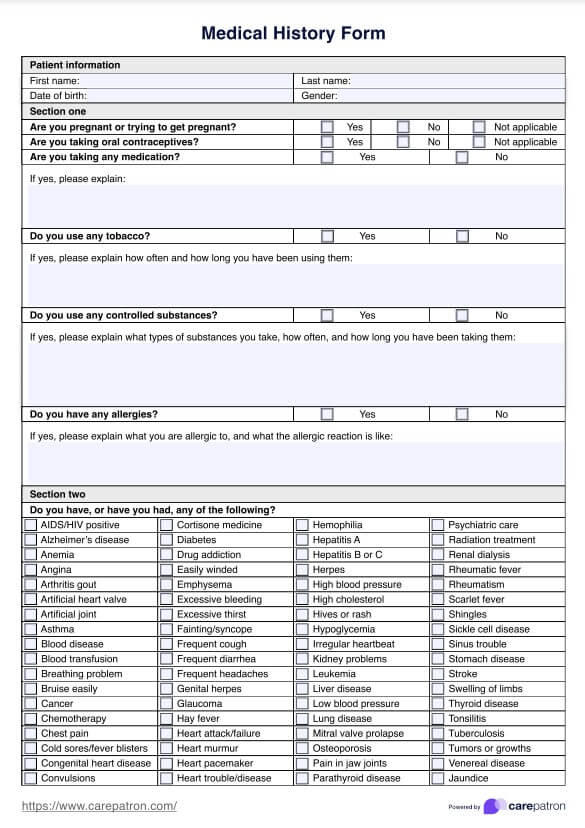
A Medical History Form is a document that contains a patient's medical information. This health history questionnaire typically includes essential information such as previous diagnoses, illnesses, medication history, treatments, surgeries, allergies, visits, referrals, and other notes. Sometimes, it may include family history and demographic questions like education, marital status, race, and employment status. When they are admitted to a hospital, this may help look further into what caused a patient's chief complaint or altered mental status.
It should be comprehensive and cover any previous details that healthcare practitioners should know when evaluating patients and guiding their treatment. When working with multiple clients in one practice, it's easy to confuse the small details, so you must compile effective methods that eliminate misattributions and invalid treatments.
With the Medical History Form template, you can ensure you get the correct data whenever you cover all relevant healthcare information. You'll be able to treat patients, prioritize their needs, and consider a range of factors that could influence the efficacy of your services.









