Nursing Home Report Sheet
Download Carepatron's free Nursing Home Report Sheet PDF and organize and track information for effective nursing home care.

Fact Checked by Ericka Pingol.


What is a Nursing Home Report Sheet?
A Nursing Home Report Sheet is an essential document used by healthcare professionals to ensure consistent patient care and manage shifts effectively in nursing homes. It serves as a comprehensive record that gathers key information about each patient’s condition, facilitating clear communication and continuity of care.
Healthcare professionals, including nursing students and seasoned nurses, rely on these report sheets to record important patient data accurately. These sheets are crucial for documenting vital signs, assessing patient conditions, reviewing ongoing care strategies, and managing medication lists. They also ensure that all medical actions are noted and effectively communicated to the next shift, reducing errors and improving outcomes.
Nursing Home Report Sheets are vital tools that support effective team communication, ensure the continuity and review of patient care, and enhance the efficiency of healthcare services in nursing facilities.
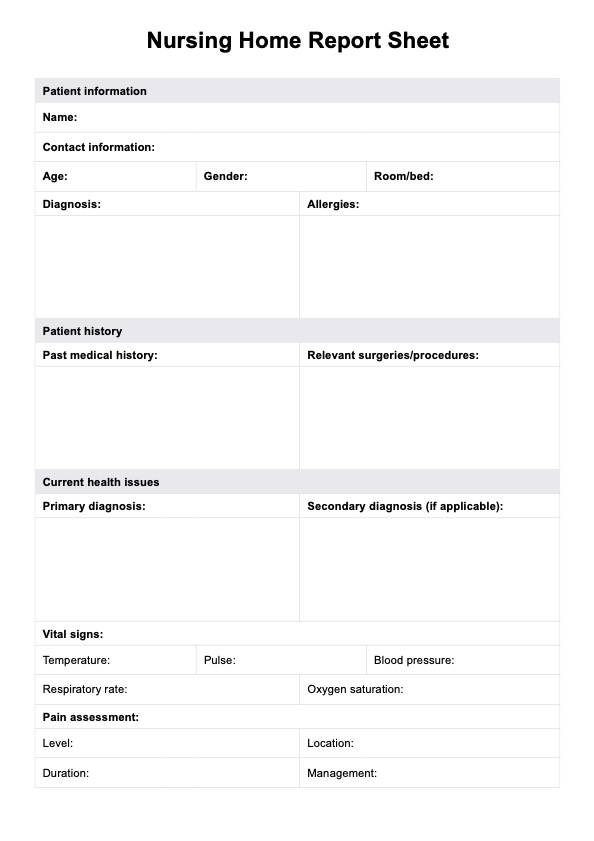
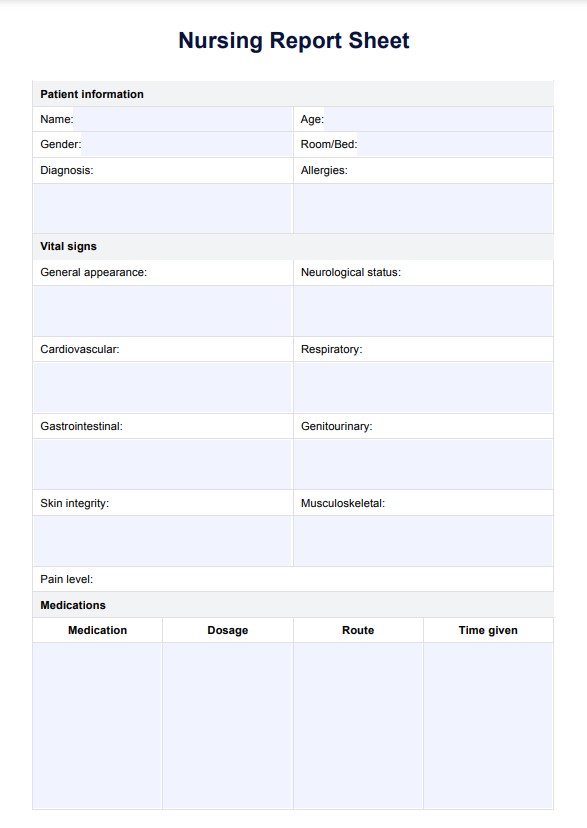
Nursing Home Report Sheet Template
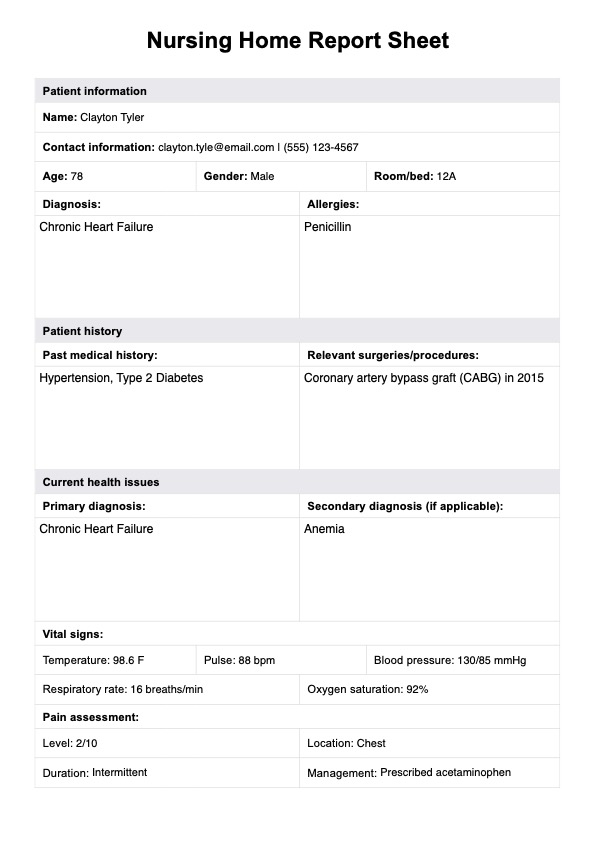
Nursing Home Report Sheet Example
Key components of a Nursing Home Report Sheet
A Nursing Home Report Sheet is a comprehensive tool designed to assist nurses in hospitals and care units by centralizing crucial patient information. These sheets help ensure that every nurse has the best experience and full knowledge needed to provide optimal care. Here, we break down the essential components of a Nursing Home Report Sheet.
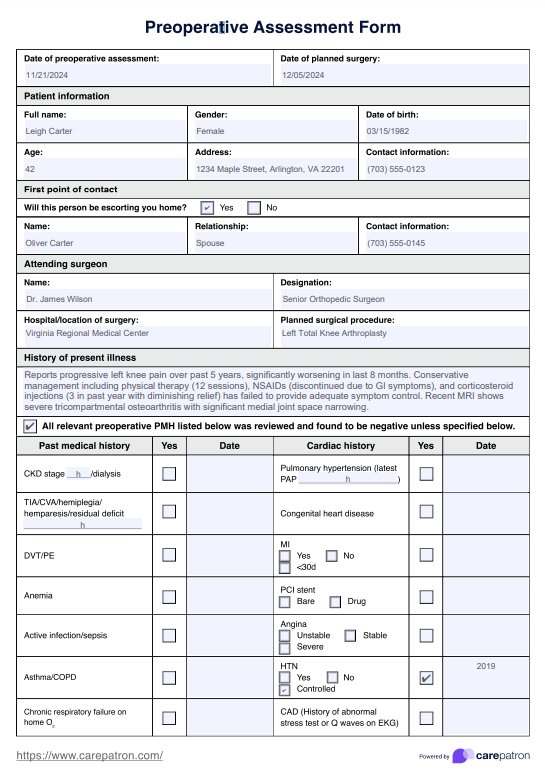
Patient information and medical history
This section contains the patient’s personal details such as name, age, and room number, along with a detailed medical history. It includes past diagnoses, surgeries, and ongoing health concerns, helping nurses quickly understand the patient's background.
Current health status and vital signs
Critical for immediate assessment, this part records the patient's current health complaints and vital signs, such as temperature, blood pressure, pulse, and respiratory rate. It helps nurses monitor changes and respond promptly.
Current medications
Here, nurses log all medications a patient is taking, including dosages, administration routes, and times. This component is vital for managing drug interactions and ensuring continuity of care across shifts.
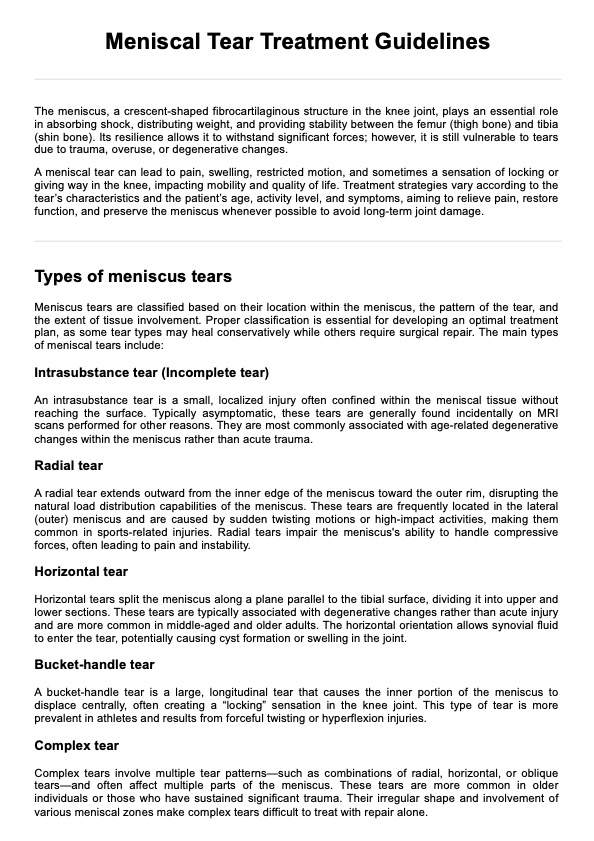
Treatments and procedures
This section outlines any ongoing or scheduled treatments and medical procedures, clearly describing care plans. It's essential for preparing staff for the patient's care needs during their shift.
Laboratory and diagnostic results
Recent lab and diagnostic results are detailed here, offering insights into the patient's condition and any necessary medical adjustments. This helps inform treatment plans and monitor progress or emerging concerns.
Activities of Daily Living (ADLs)
Assessment of the patient’s ability to perform daily activities like bathing, dressing, and eating is recorded in this part. Understanding ADL capabilities is crucial for tailoring nursing care to the patient's needs.
Care plan and interventions
This final component outlines the nursing diagnosis and planned interventions, ensuring every team member is aware of the patient’s care objectives and the strategies in place to address them. It facilitates coordinated care and clear communication among nursing staff.
How does it work?
Using the Nursing Home Report Sheet from Carepatron streamlines documenting and managing patient care in a nursing home setting. Here’s a step-by-step guide on how medical professionals can incorporate this tool into their daily routines.
Step 1: Access the template
Click "Use template" to open and customize the Nursing Home Report Sheet in the Carepatron app. The template is easy to modify, featuring fillable tables and sample data for everyday use, ensuring you can tailor it quickly to meet your specific needs. For a PDF copy, choose "Download."
Step 2: Utilize the report sheet in your workflow
Once you have the template, integrate it into your daily routine. Use it to record patient information at the start of your shift or when assessing new patients, ensuring all critical data is captured accurately.
Step 3: Use the gathered report for further patient assistance
The information collected on the Nursing Home Report Sheet should be used to assist in making informed decisions about patient care. This data helps track progress, monitor changes, and coordinate activities with other healthcare professionals.
Step 4: Keep reports for patient records
Completed report sheets should be kept as part of the patient’s medical records. This ensures a comprehensive history is available for future reference, aiding in ongoing patient care and any necessary medical reviews.
Benefits of using this report sheet
Using the Nursing Home Report Sheet provides significant benefits for medical professionals, enhancing patient safety and improving the efficiency of healthcare delivery.
One of the primary advantages is the streamlined process of documentation. This report sheet allows nurses to quickly search for and access patient information, ensuring that all data—from vital signs to treatment plans—is updated in real-time and easily available. The ability to sign and print the report directly from the system not only saves time but also reduces the likelihood of errors, as the description of patient conditions and prescribed interventions are clearly documented and can be consistently followed by all team members.
Additionally, creating a standardized output that can be signed off by attending healthcare providers ensures that each patient's care is thoroughly reviewed and endorsed, enhancing accountability and continuity of care. By using these nursing report sheets, medical professionals can focus more on patient care rather than administrative tasks, leading to better health outcomes and a more organized work environment.
Commonly asked questions
To create a nursing report sheet, start by including all essential patient information, such as demographics, medical history, current condition, and treatment plans. Ensure it is organized for quick access and updates, making it practical for use during shifts.
When writing a nursing report, clearly document the patient's current health status, any changes observed, interventions made, and the response to those interventions. It's important to be concise and accurate to ensure that the report is useful for subsequent care providers.
A nursing report typically includes sections on the patient’s identification, medical history, vital signs, assessments, treatments, and any notable changes in their condition. It should also detail the nursing interventions performed and any planned follow-up care.
Related Templates

Popular Templates