Nursing Report Sheets
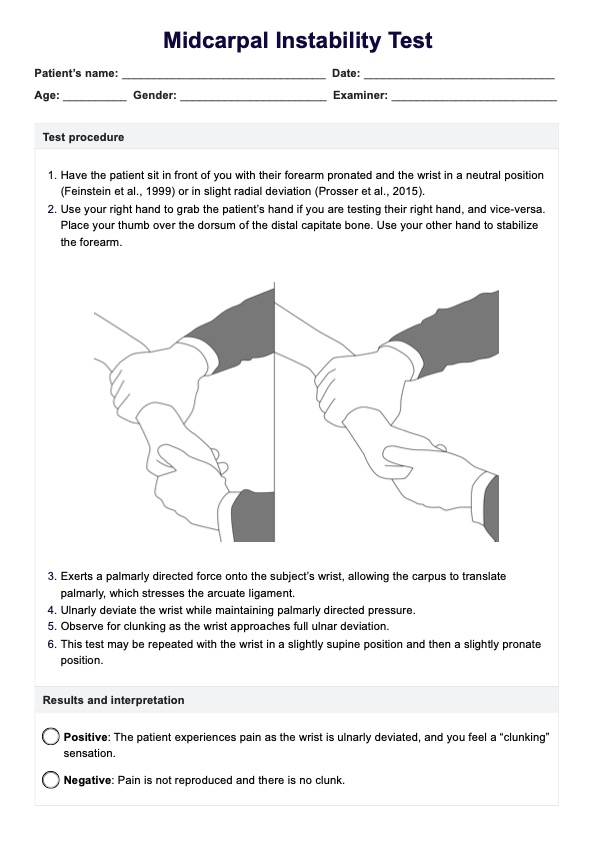
Understand the key components of Nursing Report Sheets and the best practices for using them.

Fact Checked by Ericka Pingol.


What is a Nursing Report Sheet?
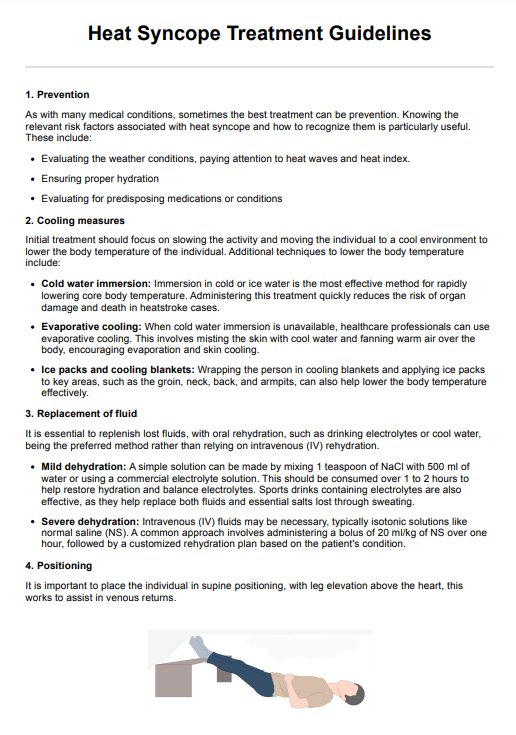
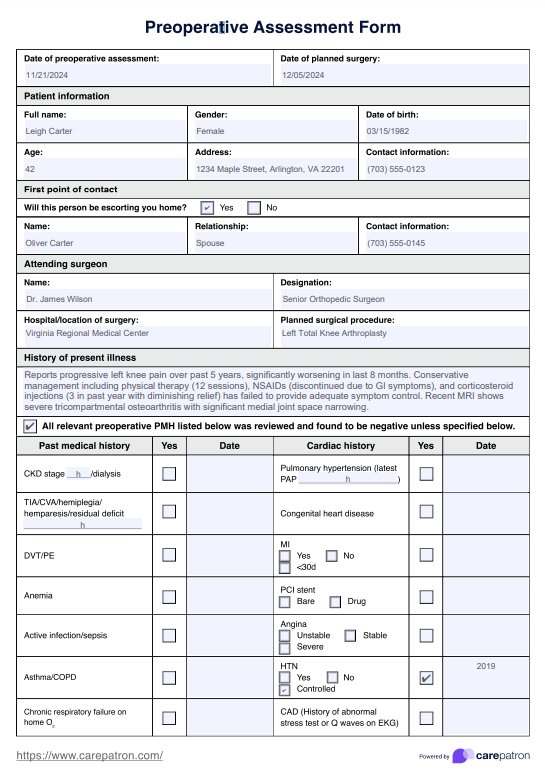
A Nursing Report Sheet, also known as a nursing brain sheet or patient report form, is a comprehensive document that healthcare professionals use to communicate all the details about a patient's condition, treatment plan, and progress during shift changes or when transferring the patient between units or facilities.
Documenting through brain sheets is vital for ensuring continuity of care and effective communication among nurses, even nursing students, and other healthcare providers. This report sheet typically contains several sections that capture the patient's medical history, current condition, and ongoing care.
These sheets are especially helpful for nursing students or new nurses, as they serve as beneficial education tools. A nurse educator can use them to help students learn how to prioritize important information, communicate effectively with other healthcare professionals, and stay organized during their clinical rotations or job experiences, even in early nursing school.
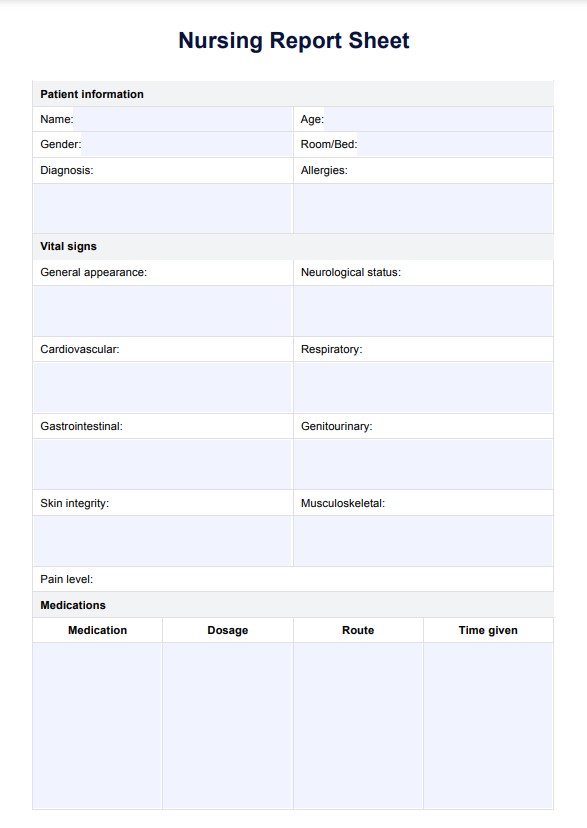
Nursing Report Sheets Template
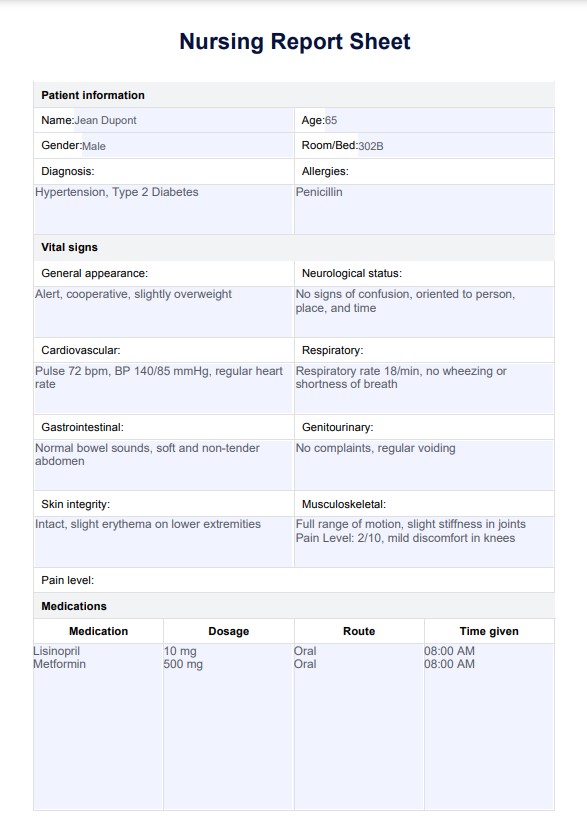
Nursing Report Sheets Example
How does it work?
Our printable Nursing Report Sheet PDF is divided into various sections to make filling it out easier. The sections include patient information, medications, vital signs, and assessments. Here's how to get started with this free template:
Step 1: Obtain a copy
The free nurse report sheet template can be downloaded using this page's link or the Carepatron software. It is also available in our extensive resources library where you can have free downloads of other templates.
Step 2: Enter patient information
Enter the patient's name, age, and other relevant personal information. Then, enter the patient's medical history, including any chronic conditions or medications they take.
Step 3: Record relevant details
Use the template to record the patient's vital signs, lab results, interventions, and other pertinent information. List any treatments or medications the patient takes and their response to them.
Step 4: Save your report sheets
Once you have completed the Nursing Report Sheet, save it securely. This will make it easy to refer to the patient's information.
When would you use this Nurse Report Sheet?
You can use the Nurse Report Sheets to provide a patient assessment and care plan. This includes admissions, follow-up visits, post-operative assessments, and other scenarios. This form makes giving report convenient. Moreover, it is particularly used to:
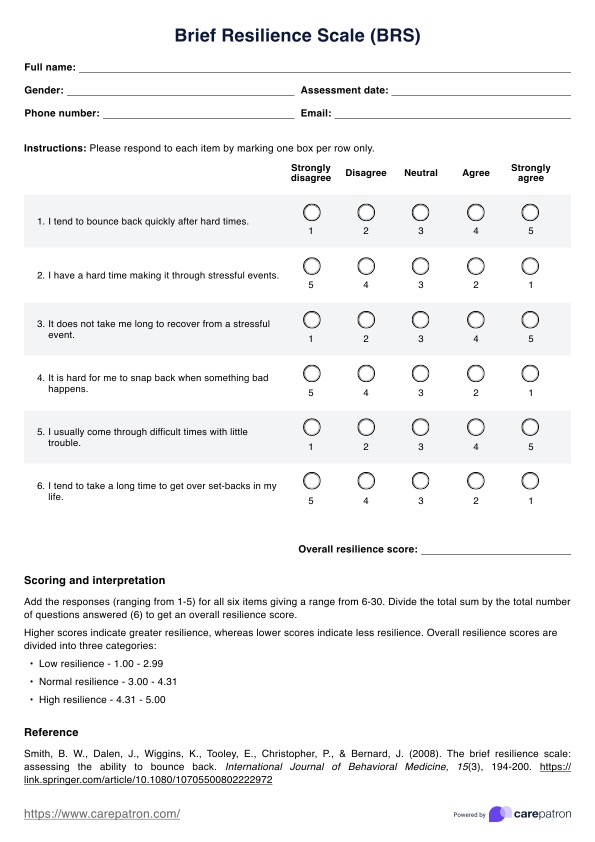
Monitor vital signs
Using a Nursing Report Sheet, you can easily track and record a patient's vital signs, such as heart rate, blood pressure, respiration, temperature, etc. This information can help you create a comprehensive picture of the patient's health condition, especially for an ICU nurse, where this information is crucial.
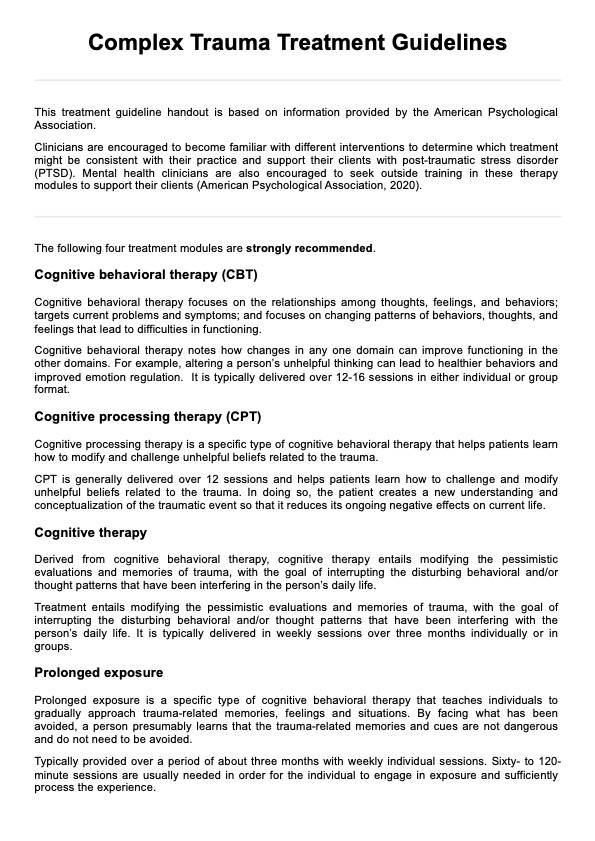
Document interventions
When assessing patients, it's essential to document any interventions or treatments performed, whether by old or new nurses. A Nursing Report Sheet can help you keep track of all the steps taken to ensure a patient's safety and well-being.
Provide a comprehensive overview for other medical professionals
This template can provide a comprehensive overview for other medical professionals who may consult on the patient's care. This can help ensure that the patient receives the best possible care.
Keep a secure record of patient information
The Nursing Report Sheet is an easy way to store patient information securely and confidentially. It can help you monitor important information when giving a report.
Benefits of using a Nursing Report Sheet
Using a Nursing Report Sheet offers numerous benefits, especially ensuring patient safety and facilitating effective communication among healthcare professionals in a clinic or hospital. Here are some key advantages:
Promoting patient safety
Nursing Report Sheets help minimize the risk of medical errors by accurately documenting and sharing all relevant information about a patient's condition, treatment plan, and progress. This enhances the quality of patient care and helps prevent potential adverse events.
Streamlining handoff communication
They provide a structured way to communicate crucial details to the oncoming nurse during shift changes or when transferring patients between units or facilities. This ensures that vital information about the patient's condition and ongoing care is not missed or misinterpreted.
Enhancing continuity of care
A nurse shift report sheet enables experienced nurses and those new to the case to quickly understand the patient's situation and provide appropriate care by outlining a comprehensive overview of the patient's medical history, current condition, and treatment plan.
Promoting organization and efficiency
A report sheet for nurses is a central repository for all relevant patient information, allowing nurses to stay organized and efficiently manage their tasks and responsibilities during their shifts.
Facilitating documentation
Many hospitals and healthcare facilities require these report sheets for nurses as part of their documentation processes. These sheets provide a standardized format for capturing essential patient data, ensuring consistency and completeness in medical records.
Using medical records, care plans, and client list templates can elevate your practice and improve client success. These templates provide a systematic approach to documentation, care planning, and client management.
Commonly asked questions
A nursing brain sheet is a tool nurses use to organize and prioritize patient care tasks during a shift. It is a concise and structured document that outlines the patient's current status, medications, treatments, and any changes or concerns. The brain sheet helps nurses stay focused and ensure all necessary tasks are completed during the shift.
A nursing report should include all relevant information about the patient's current status, including vital signs, medications, treatments, and any changes or concerns. The report should also include the patient's medical history, allergies, and relevant test results or laboratory values.
A nurse-to-nurse report sheet is used during shift changes to communicate essential patient information between outgoing and incoming nurses.
Related Templates

Popular Templates

-template.jpg)