The Gartland classification of supracondylar fractures is a system used to categorize the severity of humeral fractures in children, specifically focusing on extension-type supracondylar fractures based on the degree of displacement and stability.
Gartland Classification
Explore our guide on the Gartland Classification system for classifying and managing supracondylar humerus fractures effectively.

Use Template
Gartland Classification Template
Commonly asked questions
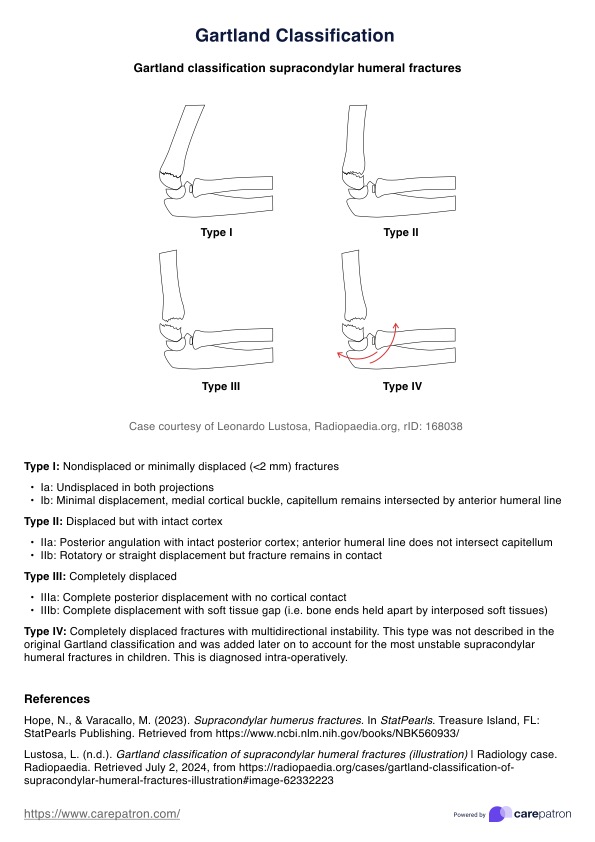
Treatment for supracondylar fractures varies: Type I fractures typically require casting, Type II fractures may need closed reduction and casting or pinning, and Type III fractures usually necessitate surgical intervention with open reduction and internal fixation.
A supracondylar fracture classification is a system wherein a displaced supracondylar fracture is given a type depending on its severity. It helps healthcare providers determine the severity of extension-type supracondylar fractures and guides the appropriate treatment approach, influencing the decision between non-surgical and surgical interventions.










EHR and practice management software
Get started for free
*No credit card required
Free
$0/usd
Unlimited clients
Telehealth
1GB of storage
Client portal text
Automated billing and online payments