Case Management Notes
Produce well-written case notes with tips from our guide and a free Case Management Notes template.

Fact Checked by Nate Lacson.


What are case notes?
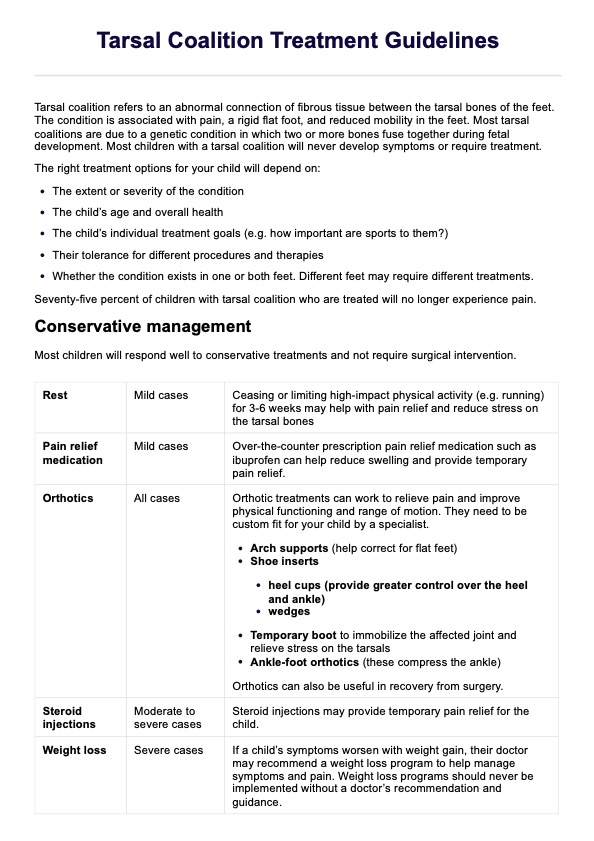
Case notes or Case Management Notes are integral to the client care process in social services and healthcare. These records, created by a case manager or social workers, serve as comprehensive documentation of a client's journey, covering their history, goals, and responses to treatment. These notes play a role in the assessment, planning, and evaluation of services tailored to meet the unique needs of each client within the social and healthcare context.
A well-crafted case management note adheres to key principles, ensuring its effectiveness in enhancing the overall quality of care. It must be accurate and complete. Clarity and conciseness are essential, focusing on information directly relevant to the established goals for case management. Timeliness is a critical factor, as the note should be completed in a timely manner to maintain the continuity and accuracy of the client's record.
Beyond aiding case managers, these records assist investigators in compiling data, finding patterns, and identifying information for a more comprehensive treatment plan. In essence, Case Management Notes emerge as pivotal instruments in facilitating informed decision-making and promoting the optimal well-being of individuals in need.
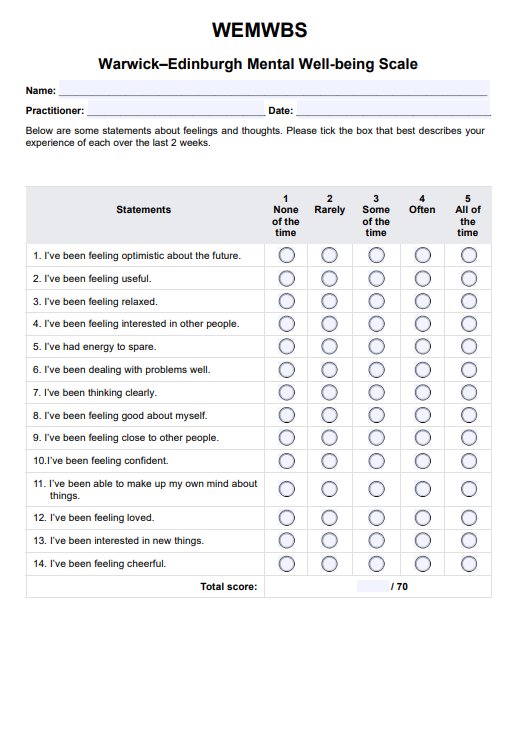
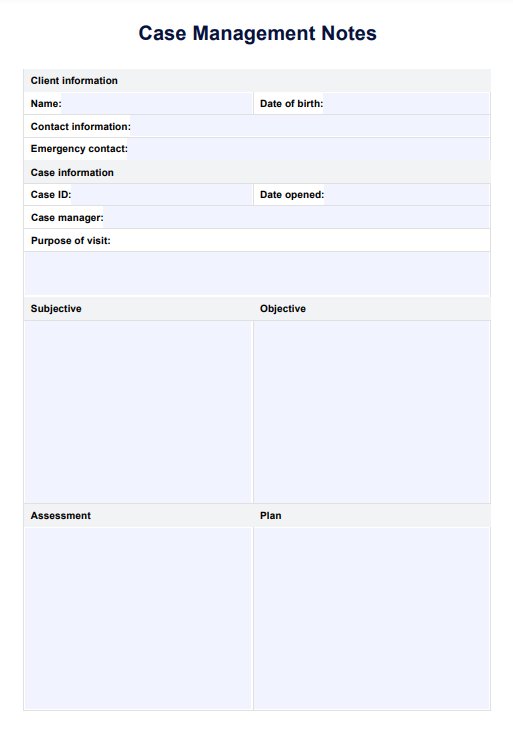
Case Management Notes Template
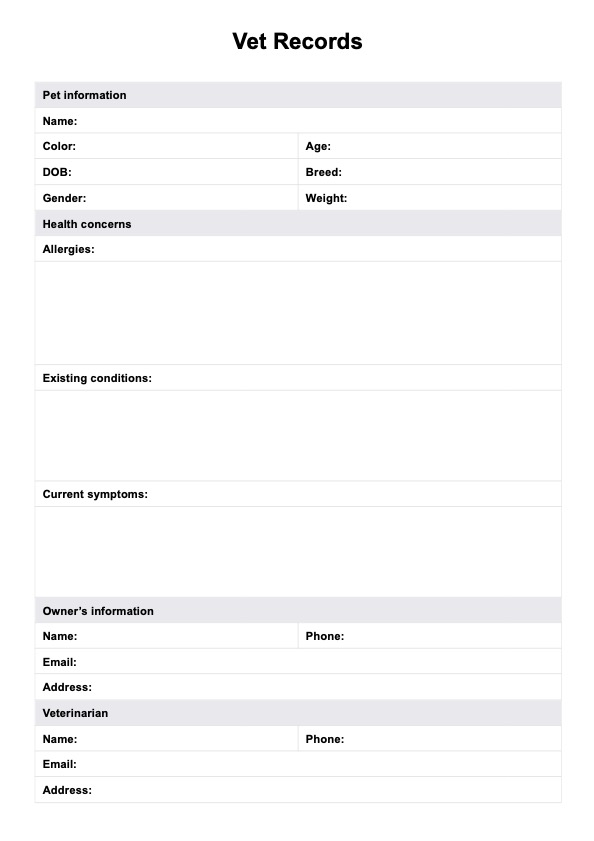
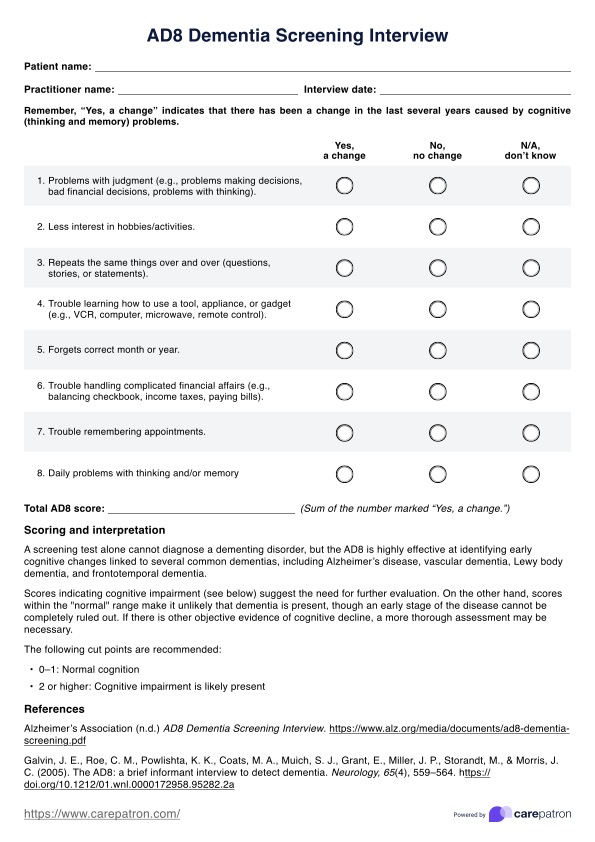
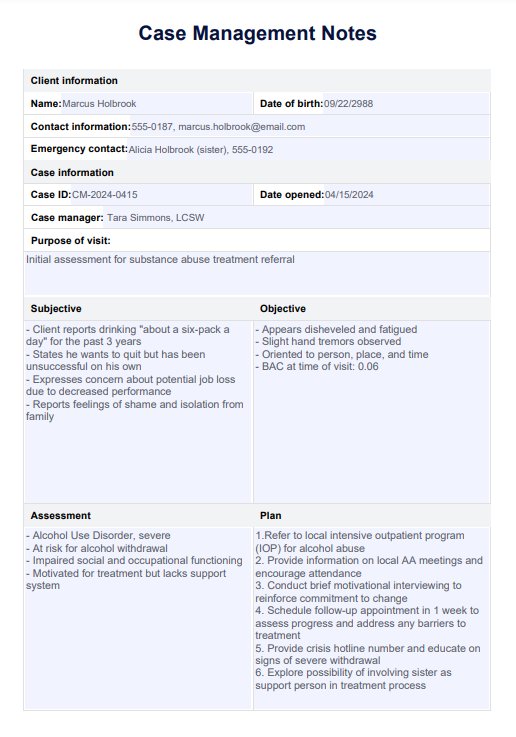
Case Management Notes Example
How to use Case Management Note template?
We have created case note templates to help streamline clinical documentation. A licensed clinical social worker can use this template aims to case workers write Case Management Notes. Here's a short step by step guide to use this resource:
Step 1: Select and download the template
Start by choosing a Case Management Notes template that aligns with your organization's requirements and the nature of your services. You can find one within this guide and download it by clicking the "Download Template" or "Use Template" button. Aside from those, you can also find this case notes templates in Carepatron's template library. It can also help to download the sample case notes to serve as a guide on how to complete it.
Step 2: Fill out the sections
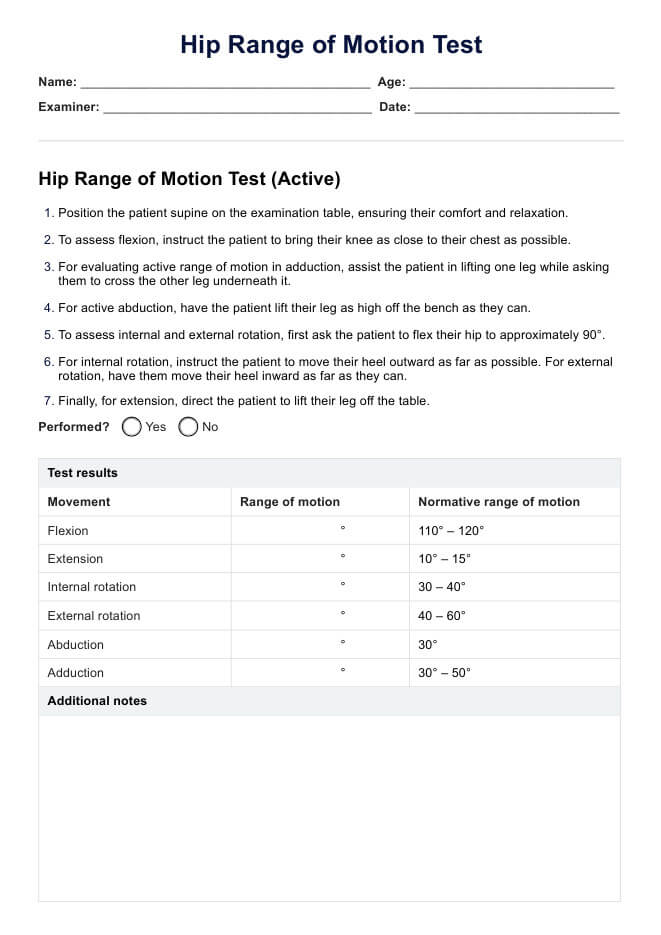
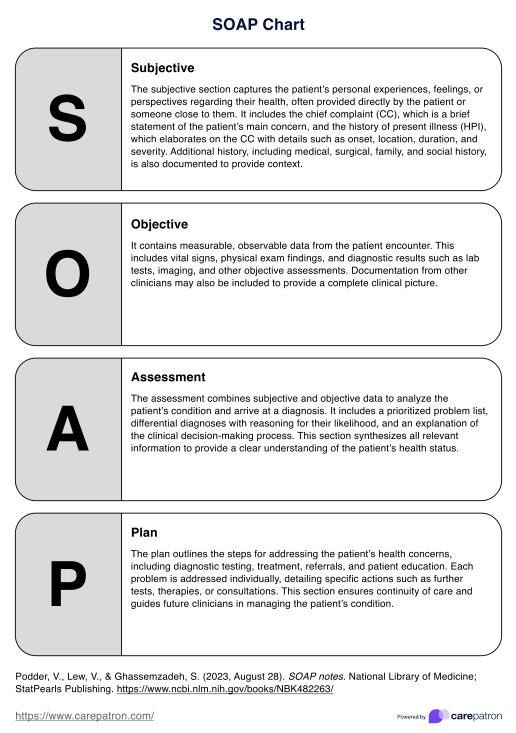
Since our case note recording template follows the SOAP format, as you're writing case notes, ensure that you fill out the Subjective (client's appearance, chief complain etc.), Objective (measurable and observable observations), Assessment, and Plan (treatment goals, planned interventions) sections.
Step 3: Review and edit
For proper case note management, it's important to first review the entire document for clarity, accuracy, and completeness. Ensure that the language is professional and the information is organized logically.
Step 4. Save and store securely
Save the completed case note template in a secure and accessible medical records software or case management software like Carepatron. This can help you manage case notes and critical client information while remaining efficient and compliant with the Health Insurance Portability and Accountability Act (HIPAA).
Besting practices for writing case notes
To write case notes, it is essential to ensure accuracy and including a comprehensive record of client interactions. Here are some best practices for writing and recording case notes:
- Be accurate and complete: Thoroughly document accurate and complete information. Missing or inaccurately entering client details can compromise the effectiveness of the notes.
- Be clear and concise: Prioritize clarity over verbosity. Focus on essential facts and pertinent details to ensure concise and effective communication, avoiding unnecessary information.
- Make notes readable and chronological: Organize case notes in a readable and chronological order, facilitating easy reference and understanding of the client's progression over time.
- Be clear about goals and objectives: Clearly state the client's goals and objectives in your notes. This provides a strategic framework for understanding the purpose and direction of the intervention.
- Use professional, plain language and an objective tone: Utilize professional and straightforward language, incorporating correct capitalization and punctuation. Maintain an objective tone that avoids biases and reflects the seriousness and professionalism of your role.
- Stick to the facts: Document only observable facts, direct quotations, and clear details. Avoid speculative information and maintain a commitment to factual and evidence-based reporting.
Benefits of using our Case Management Notes template
Our Case Management Notes template offers several advantages that can streamline your workflow, enhance communication, and improve overall patient outcomes. This includes the following:
Standardized documentation
The template provides a consistent format for recording patient information, ensuring that all essential details are captured systematically. This standardization helps reduce errors and omissions, making it easier to track patient progress over time.
Time efficiency
With a structured approach to note-taking, the template can significantly reduce the time spent on documentation. Healthcare practitioners can quickly fill in relevant sections, allowing more time for direct patient care and other critical tasks.
Improved communication
Our case notes template facilitates clearer communication among healthcare team members. It ensures that all pertinent information is readily available and easily understood, promoting better coordination of care.
Enhanced care continuity
With a comprehensive and easy-to-follow format, the template supports seamless care transitions. When patients move between different healthcare settings or providers, the standardized notes help ensure continuity of care, better treatment outcomes, and reduce the risk of information loss.
Legal and regulatory compliance
This social work case notes template is designed to meet legal and regulatory requirements for healthcare or social work documentation. This can help protect both practitioners and healthcare organizations in case of audits or legal challenges.
Commonly asked questions
Case management documentation refers to the systematic recording of information related to a client's case, including assessments, service plans, interventions, and outcomes. This documentation is essential for tracking the progress of clients, ensuring continuity of care, and facilitating communication among healthcare providers. It serves as a legal record and helps in evaluating the effectiveness of interventions and services provided.
Case notes should include key information such as the date of the encounter, client’s identifying information, the client's subjective thoughts, objective observations made by the case manager, any assessments conducted, and the outcomes of interventions. Additionally, notes should document any changes in the client’s situation, follow-up actions required, and plans for future meetings or services.
To write a good case management progress note, start with a clear and concise summary of the client’s current status and any significant changes since the last note. Use objective language and avoid jargon to ensure clarity. Include specific details about interventions implemented during the session, the client’s response to those interventions, and any goals achieved or challenges encountered. Finally, outline next steps or recommendations for future care, ensuring that the note is well-organized and easy to follow.
Related Templates

Popular Templates