Scratch Collapse Test (SCT)
Learn about the Scratch Collapse Test (SCT), a clinical assessment for nerve compression syndromes like carpal tunnel and cubital tunnel syndrome.

Fact Checked by Nate Lacson.


What is carpal tunnel syndrome?
Carpal tunnel syndrome (CTS) is a prevalent condition characterized by numbness, tingling, and pain in the hand and forearm. It arises from peripheral nerve compression, specifically when the median nerve is squeezed as it traverses through the wrist (Orthoinfo, 2022). The diagnosis of carpal tunnel syndrome is critical due to its progressive nature, which can lead to permanent hand dysfunction if untreated.
Symptoms
Recognizing symptoms is crucial for healthcare professionals to diagnose and manage CTS effectively. Here are the key symptoms:
- Numbness, tingling, burning, and pain: These sensations primarily affect the thumb, index, middle, and ring fingers and often disrupt sleep (Orthoinfo, 2022). This symptom is a primary indicator in the diagnosis of CTS, distinguishing it from cubital tunnel syndrome, which affects the ulnar nerve.
- Shock-like sensations: Patients may experience occasional shock-like sensations radiating to the thumb and fingers.
- Weakness and clumsiness: Weakness and clumsiness in the hand can hinder fine motor tasks, such as buttoning clothes, due to impaired median nerve function.
- Gradual onset: Symptoms often begin gradually without specific injury. Initially intermittent, they become more frequent and persistent over time.
- Nighttime symptoms: Many patients wake up due to symptoms, as sleeping with bent wrists exacerbates them.
- Daytime triggers: Activities involving prolonged wrist flexion or extension, such as using a phone or driving, can trigger symptoms.
Causes and complications
Understanding the causes of CTS is essential for effective management. Key causes include:
- Heredity: Anatomical differences, such as a naturally smaller carpal tunnel, can be inherited, increasing CTS risk.
- Repetitive hand use: Repeating hand and wrist motions over long periods can cause tendon swelling, putting pressure on the median nerve.
- Hand and wrist position: Activities involving extreme flexion or extension of the hand and wrist increase pressure on the median nerve, potentially leading to maximal nerve compression.
- Pregnancy: Hormonal changes during pregnancy can cause swelling and increase pressure on the median nerve.
- Health conditions: Conditions like diabetes, rheumatoid arthritis, and thyroid imbalances can lead to CTS due to inflammation or fluid retention.
If untreated, CTS can lead to severe complications:
- Permanent nerve damage: Prolonged pressure on the median nerve can cause irreversible damage, highlighting the need for prompt diagnostic tests.
- Muscle atrophy: Severe CTS can cause thenar muscle atrophy, reducing hand strength and dexterity.
- Chronic pain and dysfunction: Persistent CTS can result in chronic pain and reduced hand and wrist function, impacting daily activities.
- Reduced functional capacity: Long-term CTS can permanently reduce hand and wrist function, affecting a patient's ability to perform daily tasks.
Scratch Collapse Test (SCT) Template
Scratch Collapse Test (SCT) Example
What is cubital tunnel syndrome?
Cubital tunnel syndrome is a condition caused by the compression of the ulnar nerve at the elbow, leading to numbness, tingling, and pain in the forearm and hand. It is the second most common peripheral nerve compression syndrome. (American Society for the Surgery of the Hand, (n.d.))
Symptoms
Here are the symptoms of cubital tunnel syndrome:
- Numbness and tingling: Patients often experience numbness and tingling in the ring and little fingers, especially when the elbow is bent.
- Pain: Pain may be felt in the elbow, forearm, and hand, often worsening at night.
- Weakness: Weakness in the hand, particularly in the grip and fine motor skills, is common.
- Clumsiness: Patients may notice increased clumsiness in hand movements.
- Muscle Atrophy: In severe cases, muscle wasting in the hand, particularly the small muscles, can occur.
Causes and complications
These are the lists of causes and complications of cubital tunnel syndrome:
- Repetitive elbow flexion: Frequent elbow bending can stretch and irritate the ulnar nerve.
- Direct pressure: Leaning on the elbow can compress the ulnar nerve.
- Anatomical variations: Variations in the elbow structure can increase susceptibility.
- Injury: Trauma to the elbow can lead to ulnar nerve compression.
What is the Scratch Collapse Test (SCT)?
The Scratch Collapse Test (SCT) is a clinical test designed to diagnose peripheral nerve compression syndromes, including carpal tunnel syndrome. This test is especially useful when other common diagnostic tests, such as Tinel’s sign and Phalen’s maneuver, yield ambiguous results.
The SCT has shown promise in identifying CTS and proximal median nerve entrapment when diagnostic clarity is needed, making it a great new clinical test for diagnosing peroneal nerve compression and multilevel ulnar nerve compression.
The SCT's sensitivity and specificity are important factors in its utility, providing a valuable clinical test for suspected carpal tunnel syndrome and other nerve compression disorders. The Scratch Collapse Test performed well in Huynh and colleagues' 2018 study that uses the Quality Assessment of Diagnostic Accuracy Studies tool (specifically QUADAS-2) with electromyography as the reference standard diagnostic test. This study supports its diagnostic accuracy and low risk of bias, making it an adequate screening test for suspected carpal tunnel syndrome and cubital tunnel syndrome.
How is this test conducted?
The SCT assesses peripheral nerve compression syndromes, including carpal tunnel syndrome and cubital tunnel syndrome.
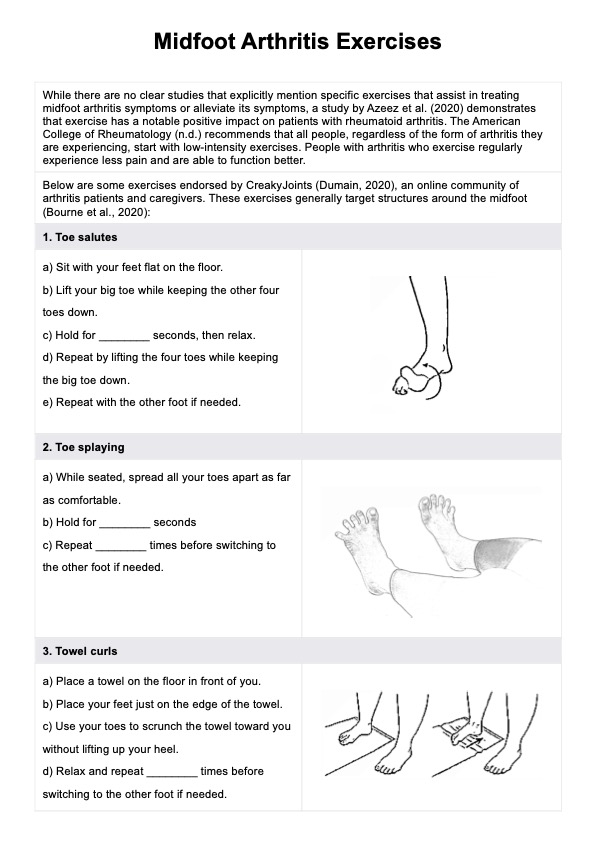
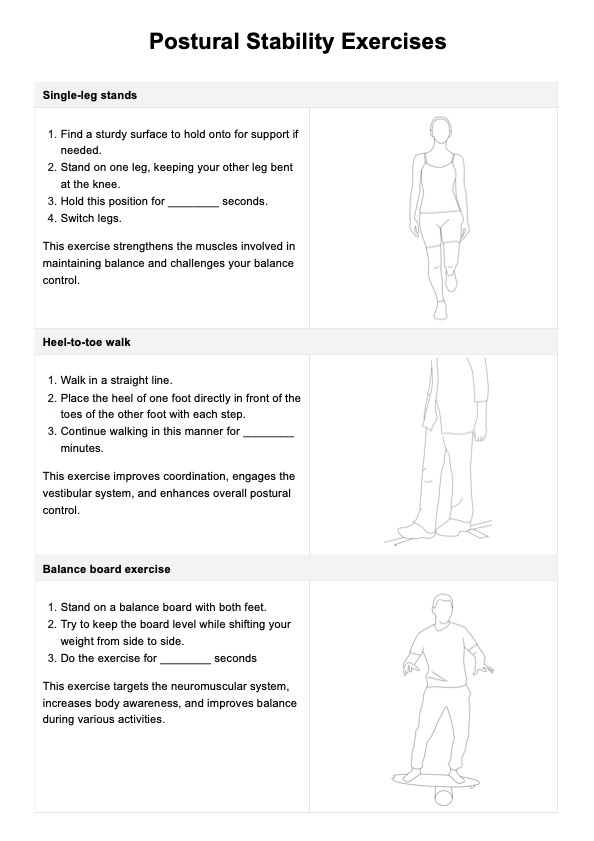
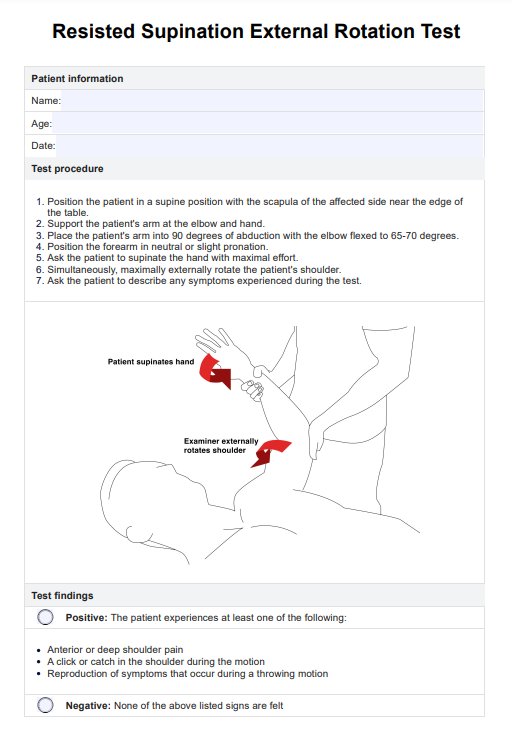
To perform the SCT:
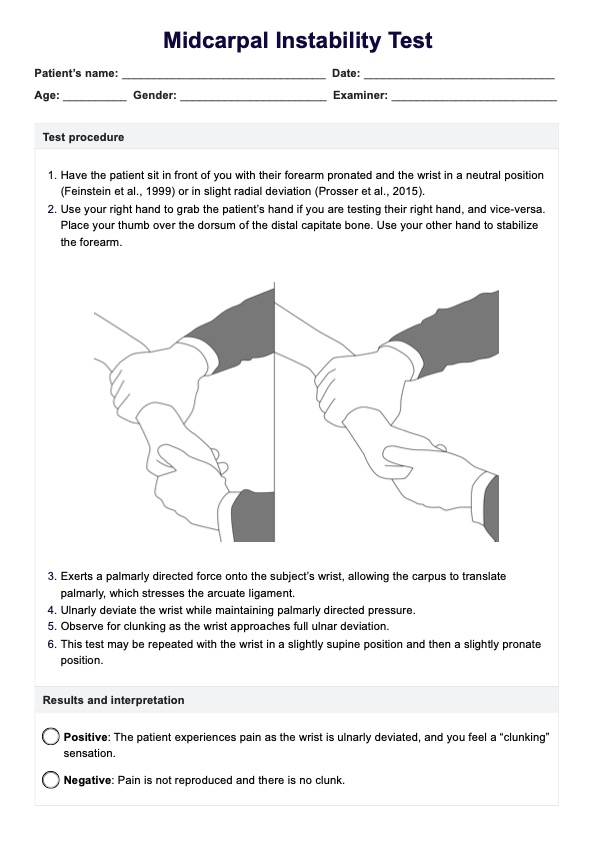
- The patient is positioned facing the examiner with both arms adducted and elbows flexed to 90 degrees, hands and wrists in a neutral position
- The examiner instructs the patient to resist bilateral shoulder adduction/internal rotation. They must only match the force you apply.
- Apply internal rotation by gently pushing both forearms inward.
- While maintaining this position, the examiner scratches or swipes the skin surface over the suspected nerve compression site.
- Immediately after, the patient is asked to resist again and apply force.
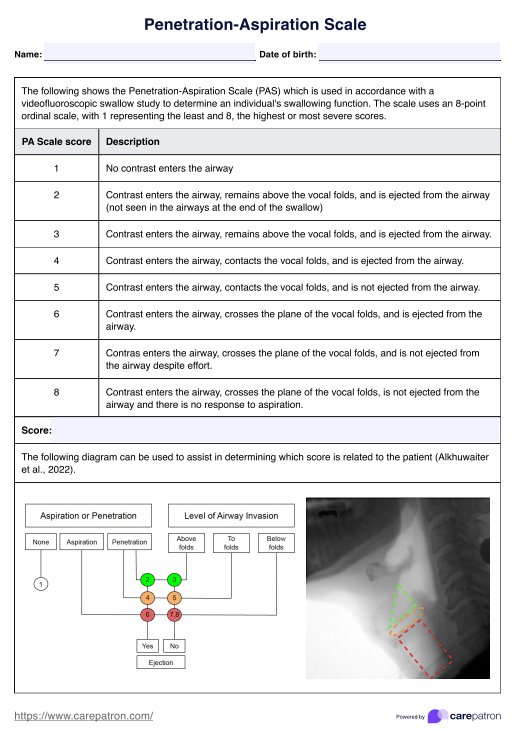
How are the results interpreted?
When interpreting the results of the SCT, orthopedic specialists observe how the patient responds during the procedure.
A positive result occurs if the patient momentarily loses muscle resistance, or their arm visibly collapses when the examiner scratches the skin over the suspected nerve compression site. This suggests potential nerve compression syndromes like carpal tunnel or cubital tunnel syndrome.
Conversely, a negative result indicates no significant muscle resistance loss or arm collapse, suggesting less likelihood of nerve compression at that site.
Next steps after conducting this test
After conducting the SCT, orthopedic specialists proceed by:
- Assess the SCT findings alongside the patient’s history and symptoms.
- Consider further tests like EMG/NCS or imaging to confirm the clinical diagnosis.
- Develop a personalized treatment plan, including splinting, therapy, injections, or surgery.
- Educate patients about their condition, treatment options, and self-care.
- Schedule regular visits to monitor progress and adjust treatment as needed for optimal recovery.
This approach ensures thorough evaluation and effective management of nerve compression syndromes.
How to use our Scratch Collapse Test template
Utilizing our SCT template facilitates structured assessment and documentation. Here are steps for using the test template:
1. Patient information
At the top of the template, enter patient details such as name, date of birth, medical record number, and date of visit.
2. Conducting the test
Administer the SCT according to the standard procedure, indicated in the template.
3. Recording findings
Document the SCT result, whether positive or negative, along with any specific affected nerve and clinical correlations observed during the test.
4. Notes and recommendations
Provide insights into the findings, discuss implications with the patient, and outline recommended next steps, such as further diagnostics or treatment options.
5. Doctor's signature
Sign and date the template to authenticate the assessment and complete the documentation process.
Benefits of conducting this test
Conducting the SCT offers several benefits in clinical practice:
- Enhanced diagnostic accuracy: The SCT has demonstrated positive results in diagnosing various nerve compression syndromes, including carpal tunnel syndrome and cubital tunnel syndrome. It provides additional diagnostic information beyond common clinical tests, potentially reducing false-positive results.
- Specificity and sensitivity: The SCT detects subtle nerve dysfunction, making it a novel test for identifying nerve compression syndromes. Compared to traditional methods, it enhances the specificity and sensitivity of diagnoses, aiding in accurate patient assessment.
- Reproducibility: The SCT is a testable and reproducible phenomenon, ensuring reliability in clinical settings. It provides standardized data collection, which is crucial for quality assessment and comparative studies using diagnostic odds ratios and negative likelihood ratios.
- Comprehensive evaluation: The SCT offers a comprehensive evaluation by assessing multiple nerve compression sites, such as the median, ulnar, and peroneal nerves. This supports differential diagnosis and appropriate management strategies tailored to each patient's condition.
- Advancement in diagnostic tools: As a novel and effective tool, the SCT contributes to advancing diagnostic capabilities in identifying nerve entrapment syndromes. Its inclusion in diagnostic algorithms alongside magnetic resonance imaging and other modalities enhances overall quality assessment data.
Common treatments for carpal and cubital tunnel syndromes
Carpal tunnel syndrome and cubital tunnel syndrome can be effectively managed through various treatments tailored to the severity of symptoms:
- Splints: Wearing wrist or elbow splints alleviate pressure.
- Lifestyle modifications: Patients with carpal tunnel or cubital tunnel syndromes should maintain their weight and avoid repetitive movements that aggravate symptoms. They should also assess and adjust their posture while working to avoid excessive strain on wrists and elbows.
- Physical exercise: There are exercises that improve nerve mobility and muscle strength. For example, nerve-gliding exercises mobilize and stretch affected nerves, helping relieve pressure and reduce pain.
- Medications: Patients with carpal tunnel or cubital tunnel syndrome can resort to non-steroidal anti-inflmmatory drugs (NSAIDs) to reduce inflammation and pain. Corticosteroid injections also provide temporary immediate relief by reducing swelling.
- Surgical interventions: Some cases require surgical procedures. One option is carpal tunnel release, which relieves pressure on the median nerve. Another option is the cubital tunnel release procedure, which decompresses the ulnar nerve at the elbow.
References
American Society for the Surgery of the Hand. (n.d.). Cubital tunnel syndrome: Signs & treatment. https://www.assh.org/handcare/condition/cubital-tunnel-syndrome
Huynh, M. N. Q., Karir, A., & Bennett, A. (2018). Scratch collapse test for carpal tunnel syndrome. Plastic and Reconstructive Surgery - Global Open, 6(9), e1933. https://doi.org/10.1097/gox.0000000000001933
OrthoInfo. (2022, March). Carpal tunnel syndrome - Symptoms and treatment. https://orthoinfo.aaos.org/en/diseases--conditions/carpal-tunnel-syndrome/
Commonly asked questions
During the Scratch Collapse Test (SCT), the patient stands facing the examiner with elbows flexed at 90 degrees. The examiner applies a scratch or swipe over the skin covering the nerve suspected of compression while the patient maintains resistance. A positive test occurs if the patient involuntarily loses resistance, indicating nerve dysfunction.
The Scratch Collapse Test (SCT) is primarily used to diagnose carpal tunnel syndrome, cubital tunnel syndrome, and other peripheral nerve entrapment syndromes like ulnar nerve compression.
While the Scratch Collapse Test (SCT) shows promise as a diagnostic tool, its reliability can vary. It is recommended as an adjunct to other clinical assessments and diagnostic tests for more accurate evaluation.
Related Templates

Popular Templates