Patient Care Report
Discover how to optimize Patient Care Reports with our guide! Our template structures all necessary information, allowing you to focus on your patients.

Fact Checked by RJ Gumban.


What is a Patient Care Report Template?
A Patient Care Report Template is a form of clinical documentation primarily used by health practitioners, such as nurses or general practitioners, to keep a thorough account of the care they provide to patients. The template offers a simple, comprehensive structure that can be implemented in patient care protocols, ensuring that all relevant information is recorded accurately and is easily accessible.
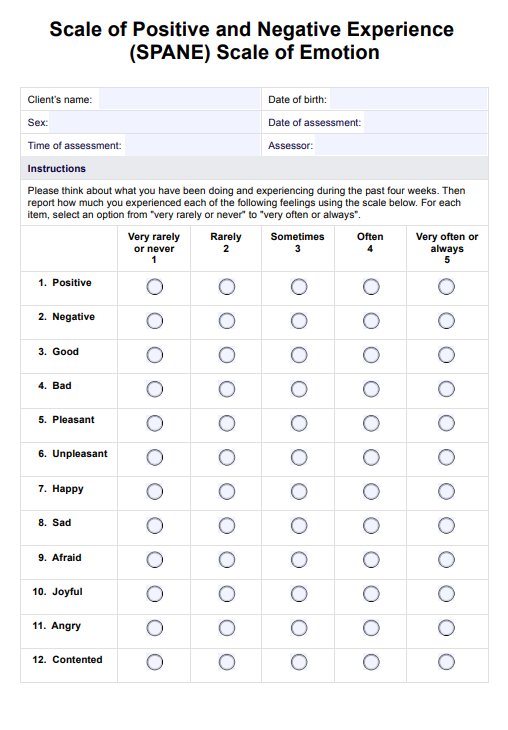
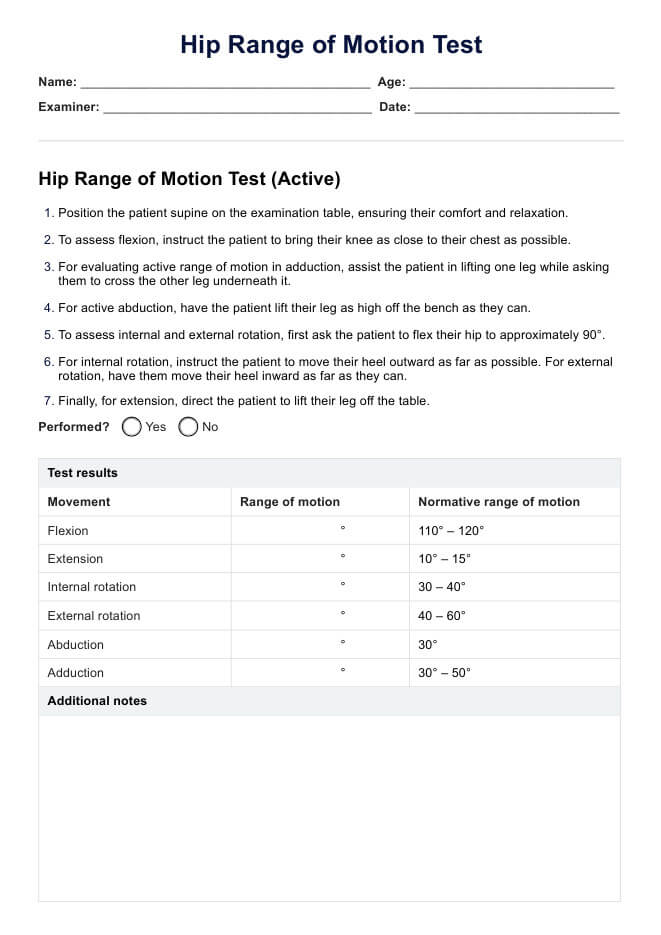
The template is customizable, so health care practitioners can use it as a reference when devising their reports or making adjustments to suit their practice. A typical patient care report template includes the following patient information:
- Patient data and medical history
- Patient's condition, current health status, and symptoms
- Source of injury or illness
- Routine and vital assessments
- Diagnostic procedures and results
The template also includes treatment information, such as:
- Treatment types and medications administered
- Patient response to treatment
- Time and date of treatment
- Health practitioners involved
The template also has a summary section that may be used as a quick reference in follow-up procedures or to communicate medical histories to other practitioners. Practitioners may also wish to record abnormal situations or responses that inform future protocols.
Our Patient Care Report Template can be accessed online or downloaded for a physical copy to be used as a procedural tool in healthcare systems, such as hospitals or emergency paramedic treatment. These are necessary to ensure accurate and thorough patient care records, which can be stored in health records and used as a reference for subsequent patient treatments.
Patient Care Report Template
Patient Care Report Example

How does it work?
Our template provides health practitioners with a structured framework on which to base their patient care reports. Here are some steps to guide you:
Step 1: Access the template
You can obtain the template on this page or download a PDF version to print a physical copy by using the button on this page or accessing it from the app.
Step 2: Fill out the patient data
Begin filling in the patient information section, including name, demographics, and contact details. Record the patient's reason for medical attention (chief complaint), including symptoms and preliminary diagnosis. Document relevant medical history, such as current allergies, injuries, or medications, which may inform diagnosis and treatment.
Step 3: Do examinations and diagnostic procedures
Accurately record the diagnostics completed, procedural details, and results.
Step 4: Start treatment
Document all treatments and protocols performed while the patient is in your care. This may include information regarding medication type, dose and frequency, and recommendations for follow-up procedures.
Step 5: Summarize and make recommendations
In the last section, summarize the patient care, including the procedures, resources, findings, and treatment provided. If the patient requires further treatment outside your care, provide referrals or recommendations. This may include any specialized diagnostic procedures or treatments, which should be described in detail.
Step 6: Review and sign
Once you have completed the report, revise the information to ensure it is thorough and accurate. Then, authorize the report's completion by signing and dating the document.
When would you use this template?
The Patient Care Report Template is a resource designed for health professionals to ensure accurate clinical documentation. Here are some appropriate uses for the template:
- Medical documentation: Healthcare professionals such as paramedics, doctors, or nurses may use the template to structure and accurately record patient information. Standardized formats are crucial, especially for EMS patient care reports, as they ensure consistency and clarity in emergency medical services.
- Organizing records: The template may support healthcare facilities like hospitals or clinics in maintaining organized patient records. These can then be implemented in the patient's medical history, informing future treatments or diagnoses.
- Insurance claims: A completed Patient Care Report may be used as evidence to confirm insurance claims. This is another form of ensuring patients are cared for and have access to their needed resources.
- Legal matters: Legal matters surrounding patient care may use the report to support or deny a particular claim. Completing a thorough report can be definitive in trials against healthcare providers, as these show competency and can reduce the guilt of health professionals in adverse circumstances.
- Inspections or improvements: These completed documents may help appraise the effectiveness of current protocols in a medical facility. An accurate report is essential for accurate assessment, which can then inform practical recommendations to enhance procedures centering patient care.
Research & evidence
Patient Care Reports are a foundational form of clinical documentation in health facilities, such as hospitals and health clinics. In understanding the value of these reports, many health practitioners perceive them to be beneficial for daily practices and ensuring safe patient care (Bjorvell et al., 2003). However, assuring the accuracy and details required for a comprehensive report can often be time-consuming.
Effective documentation relies on a universal format that is accurate, concise, and appropriate (Zierler-Brown et al., 2007). Our free Patient Care Report Template can reduce the medical errors and time spent devising care reports. With a simple structure that organizes all essential information, the template can reduce the time spent on administrative tasks, allowing practitioners to spend more time providing optimal care and improving patient outcomes.
References
Bjorvell, C., Wredling, R., & Thorell-Ekstrand, I. (2003). Prerequisites and consequences of nursing documentation in patient records as perceived by a group of registered nurses. Journal of Clinical Nursing, 12(2), 206-214. https://doi.org/10.1046/j.1365-2702.2003.00723.x
Zierler-Brown, S., Brown, T. R., Chen, D., & Blackburn, R. W. (2007). Clinical documentation for patient care: Models, concepts, and liability considerations for pharmacists. American Journal of Health-System Pharmacy, 64(17), 1851-1858. https://doi.org/10.2146/ajhp060682
Commonly asked questions
A patient care report includes pertinent information about the patient's care, such as patient demographics, medical history, current health status, treatments administered, and healthcare provider notes. Essential elements like vital signs, diagnostic results, and follow-up recommendations are also documented.
A patient care report ensures that the patient history, treatments, and outcomes are thoroughly documented. It is crucial to establish medical necessity and guide ongoing care decisions, especially in a medical emergency.
When writing a narrative for an EMS report, include detailed patient data and a chronological account of the medical emergency. Describe the patient's condition upon arrival, interventions performed, and the patient's response to treatment to provide a comprehensive overview.
Related Templates

Popular Templates