Everyone has a story to tell, and here we share and celebrate those who chose care as their life's work.
These are their words, their work and we're grateful to share them.
Elizabeth and Dennis handed their billing to Carepatron and grew My Therapeutic Concepts from five clients to seventy in two months, without losing their evenings.
Effective treatment plans ensure consistency, accountability, and progress in therapy or healthcare. This guide walks you through the process of structuring a well-organized treatment plan and utilizing our treatment plan to align goals, interventions, and outcomes with the specific needs of your patient or client.
## **What is a treatment plan?**
A treatment plan is a structured clinical document that outlines a patient’s presenting problem, diagnosis, treatment goals, and the interventions that will be used to support change or improvement. Treatment plans are used across healthcare settings, including medical, behavioral health, rehabilitation, and social care, to ensure care is consistent, coordinated, and goal-directed.
A standard treatment plan template typically includes:
- Background information (relevant medical and psychosocial history)
- The presenting problem or concern
- Measurable goals and smaller objectives
- Planned interventions matched to the diagnosis and goals
- A schedule for reviewing progress and adjusting the plan as needed
Treatment plans promote patient-centered care by involving the patient in identifying priorities and treatment goals. They also support clear communication among other healthcare providers, making continuity of care easier when multiple clinicians are involved in treatment.
## **Why treatment plans are helpful for healthcare professionals**
Treatment plans are useful beyond therapy. They support decision-making in medicine, nursing, counseling, rehabilitation, case management, community health, and more. A well-structured treatment plan:
### **Organizes care and promotes consistency**
By documenting goals, interventions, frequency of contact, and how you will measure progress, treatment plans help care stay clear and structured. This reduces guesswork and helps clinicians follow a defined care path.
### **Improves communication and collaboration**
When multiple clinicians are involved, such as physicians, therapists, nurses, or case managers, the treatment plan acts as a shared reference. This helps maintain continuity and reduces duplicated or conflicting care.
### **Strengthens clinical documentation and supports insurance requirements**
Many healthcare settings require treatment plans to justify medical necessity and demonstrate progress for reimbursement or quality review. A clear plan also provides documentation that supports legal and ethical accountability.
### **Enhances patient engagement and outcomes**
Involving patients in setting realistic, achievable goals increases motivation and follow-through. Research shows that collaborative treatment planning improves adherence and long-term symptom improvement (Bickman et al., 2016).
## **How to use this template for treatment plans**
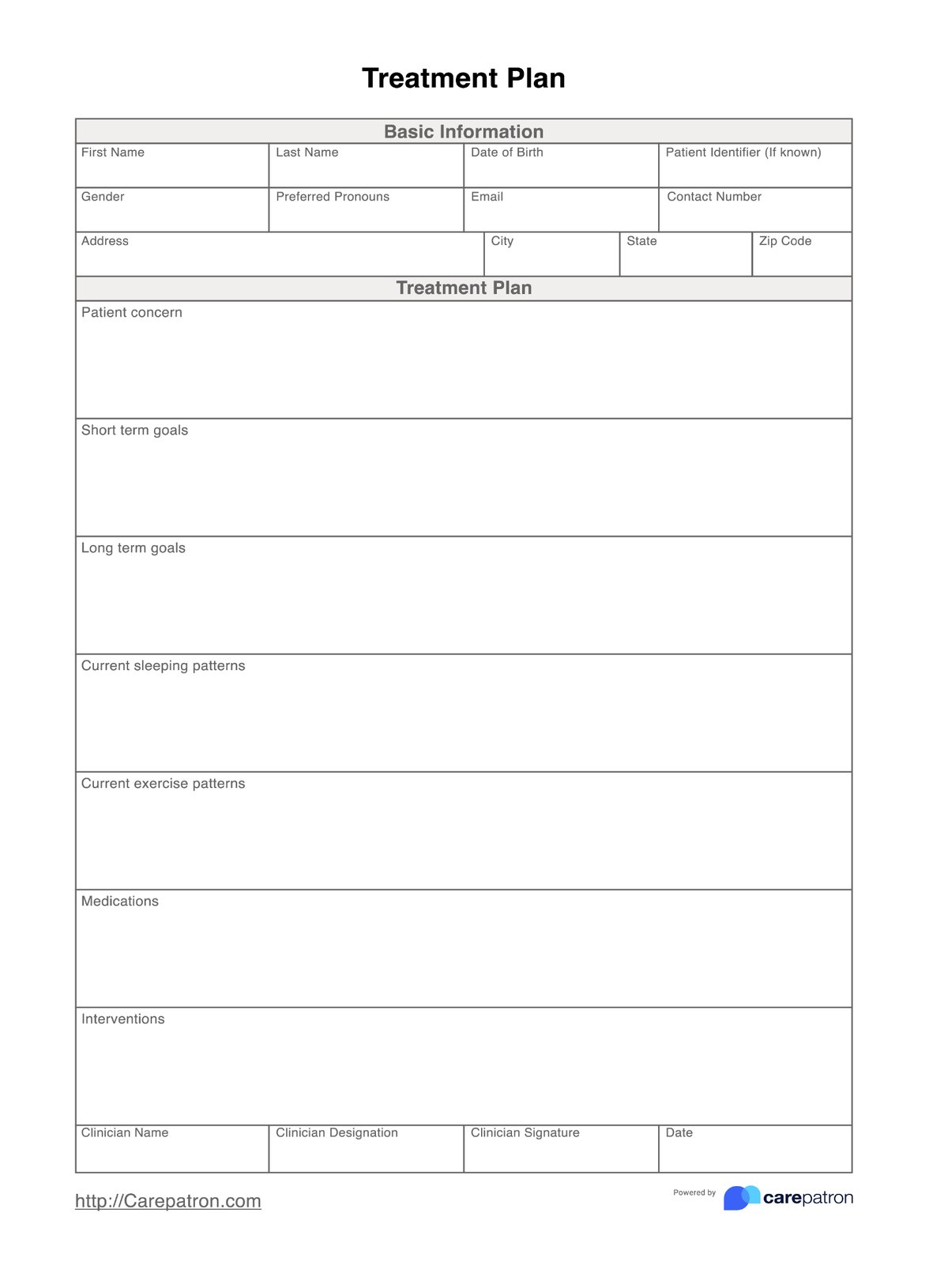
This Treatment Plan Template organizes the essentials you need to write a clear, well-structured plan. Use the layout to document the presenting problem, set SMART goals, map interventions, and track the patient’s progress over time. Follow these steps:
### **Step 1: Download the treatment plan**
Complete the demographics (name, DOB, contact, identifiers, pronouns, address) so other providers can verify identity quickly. In the patient concern, write 2–3 sentences that describe the presenting problem in plain language, including severity and duration.
Example: “Panic attacks 2–3×/week for 3 months; triggers include crowded transport; avoids grocery shopping.”
### **Step 2: Complete the treatment plan**
Use the short-term goals box for what you expect within weeks; use the long-term goals box for multi-month outcomes. Frame each as specific, measurable, achievable, relevant, time-bound, with a target metric you can evaluate.
- **Short-term example**: “Reduce panic episodes from 3×/week to ≤1×/week within 6 weeks.”
- **Long-term example**: “Resume solo grocery trips 2×/week without leaving early within 12 weeks.”
- **Tip**: Tie every intervention (Step 4) to a corresponding goal so you can measure progress at review.
### **Step 3: Document health patterns that influence treatment**
Use current sleeping patterns and current exercise patterns to capture baselines that affect symptoms and recovery. Keep these entries concrete.
Examples: “Sleep 5–6 hrs/night; 3 awakenings.” / “Walks 10 minutes, 3 days/week.”
These baselines help you evaluate change and adjust treatment goals and interventions.
### **Step 4: List medications and planned interventions**
In medications, record name, dose, frequency, indication, and notable side effects/adherence notes (e.g., “Sertraline 50 mg daily; missed ~2 doses/week; mild nausea first week”).
In interventions, specify what, how often, by whom, and for how long. Avoid vague entries. Write operational steps you can audit.
Examples:
- “CBT panic protocol: psychoeducation + interoceptive exposure 1×/week, 50 min, 8–10 sessions.”
- “Breathing drill (4-7-8) 2×/day; patient logs SUDS pre/post.”
- “Medication check with prescriber q4–6 weeks; assess PHQ-9/GAD-7.”
- “Care coordination call with PCP after 2 sessions to review BP and dizziness.”
### **Step 5: Align clinician details and dating for version control**
Complete clinician name/designation and date every time you create or update a plan. Use a consistent naming/versioning convention (e.g., “TP-Smith-2025-10-29 v2”) so your clinical documentation shows what changed and when.
### **Step 6: Review cadence and progress evaluation**
At each follow-up, compare outcomes to the short-term goal metrics you set in Step 2. Note what improved, what stalled, and why. If a goal is met, advance it; if not, revise either the goal (scope/timeline) or the interventions (frequency/method). Schedule formal plan reviews at predictable intervals (e.g., every 4–6 weeks) and whenever there’s a major change (new diagnosis, medication, risk event).
## **Other Treatment Plan Templates you may find helpful**
If you are writing treatment plans across different clinical contexts, you may benefit from additional templates that offer structure, guidance, and flexibility depending on the patient’s needs and the scope of treatment. Each option below provides key components for outlining the presenting concern, setting treatment plan goals, defining interventions, and monitoring new goals over time after a comprehensive assessment.
### **Therapy Treatment Plan template**
The [Therapy Treatment Plan template](https://www.carepatron.com/templates/therapy-treatment-plans/) is designed for mental health clinicians working with clients who are managing symptoms such as anxiety, depression, trauma responses, or emotional dysregulation. This template helps clinicians link the presenting problem to measurable progress outcomes and adjust interventions over time.
### **Counseling Treatment Plan template**
This [Counseling Treatment Plan template](https://www.carepatron.com/templates/counseling-treatment-plan/) is useful for counselors and social workers who need to establish realistic goals collaboratively with clients. It supports clarity in expectations, session direction, and communication of progress, making it suitable for individual counseling, school counseling, and community behavioral health.
### **Individualized Treatment Plan template**
An [Individualized Treatment Plan](https://www.carepatron.com/templates/individualized-treatment-plan/) is ideal when clients have complex needs that require tailored interventions involving multiple providers or support systems. This template places emphasis on person-centered care, strengths-based planning, and adapting strategies as the patient’s situation evolves.
## **Reference**
Bickman, L., Lyon, A. R., & Wolpert, M. (2016). Achieving precision mental health through effective assessment, monitoring, and feedback processes. Administration and Policy in Mental Health and Mental Health Services Research, 43(3), 271–276. https://doi.org/10.1007/s10488-016-0718-5
Commonly asked questions
A treatment plan typically includes a comprehensive overview of the patient’s presenting problem, relevant background information, SMART goals, planned interventions, progress measures, and review dates. These elements create a clear roadmap that guides treatment and helps clinicians accomplish meaningful change over time.
Use the SMART framework, which means goals should be specific, measurable, Achievable, Relevant, and Time-bound.
Example: Reduce panic attacks from 3× weekly to 1× weekly within 6 weeks.
This ensures goals are trackable and tied to observable outcomes.
Treatment plans are typically reviewed every 4–12 weeks, or sooner if symptoms, risks, or circumstances change. Updates may involve revising goals, adjusting interventions, or adding new goals based on progress evaluations.
Yes. The chosen template is flexible and can be used across therapy, counseling, medical care, rehabilitation, and community services. Its structure can be adapted to your practice needs, preferred guidelines, and clinical practices.