Disinhibited Social Engagement Disorder DSM-5 Criteria
Learn about Disinhibited Social Engagement Disorder (DSED): symptoms, treatment, and impact on children's social development in healthcare settings.

Fact Checked by Ericka Pingol.


What is disinhibited social engagement disorder (DSED)?
Disinhibited social engagement disorder (DSED) is characterized by a child's culturally inappropriate and overly familiar behavior with unfamiliar adults, stemming from experiences of social neglect or instability in caregiving. Symptoms include diminished reticence with strangers, excessive verbal or physical interaction, and a willingness to accompany unfamiliar adults. Typically emerging by age 9 months, DSED may co-occur with developmental delays and persist despite improvements in caregiving. Early diagnosis is crucial for mitigating long-term interpersonal difficulties and ensuring appropriate management tailored to the child's developmental stage and environmental context.
Disinhibited Social Engagement Disorder DSM-5 Criteria Template
Disinhibited Social Engagement Disorder DSM-5 Criteria Sample
How is disinhibited social engagement disorder diagnosed?
DSED involves a comprehensive assessment based on criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Clinicians begin by observing the child's behavior, looking for patterns such as reduced reticence with unfamiliar adults, overly familiar interactions, and a willingness to leave with strangers without hesitation (American Psychiatric Association. (2013b).
These behaviors must be contextualized within a history of severe social neglect or disrupted caregiving, which are crucial for establishing the disorder's etiology. Diagnostic tools may include structured interviews with caregivers and direct observation in various settings to assess the consistency and severity of symptoms. Differential diagnosis involves ruling out conditions like ADHD, emphasizing the distinction in social behaviors versus attention deficits.
Disinhibited Social Engagement Disorder DSM-5 Criteria
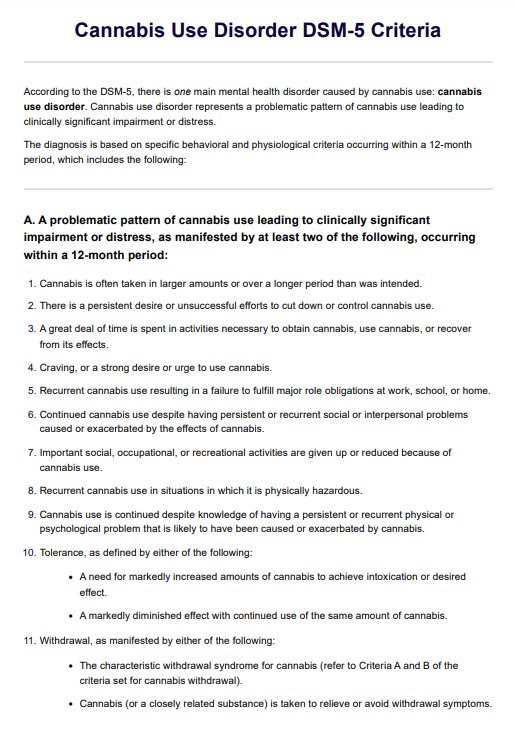
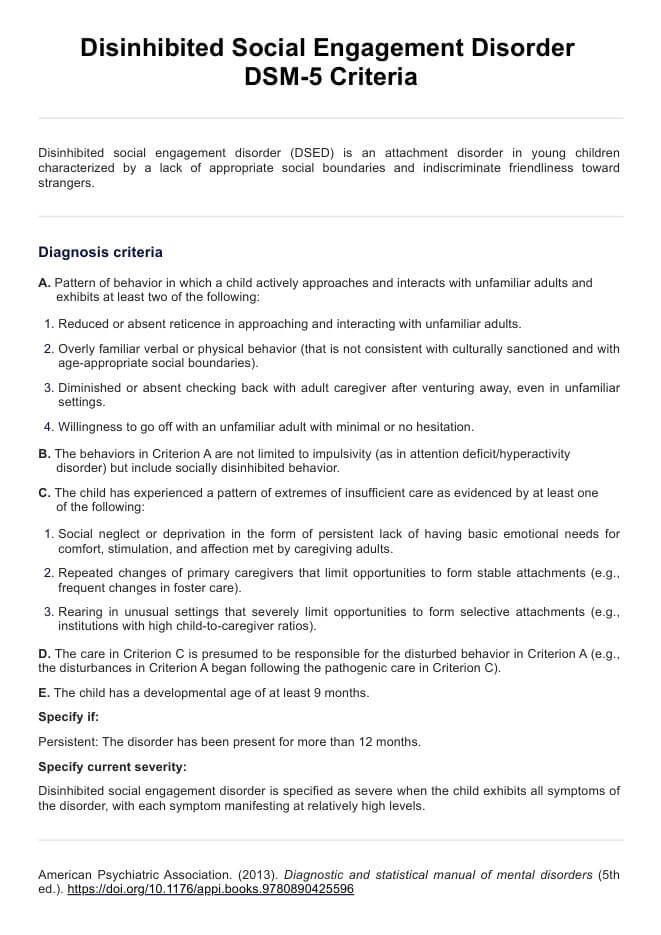
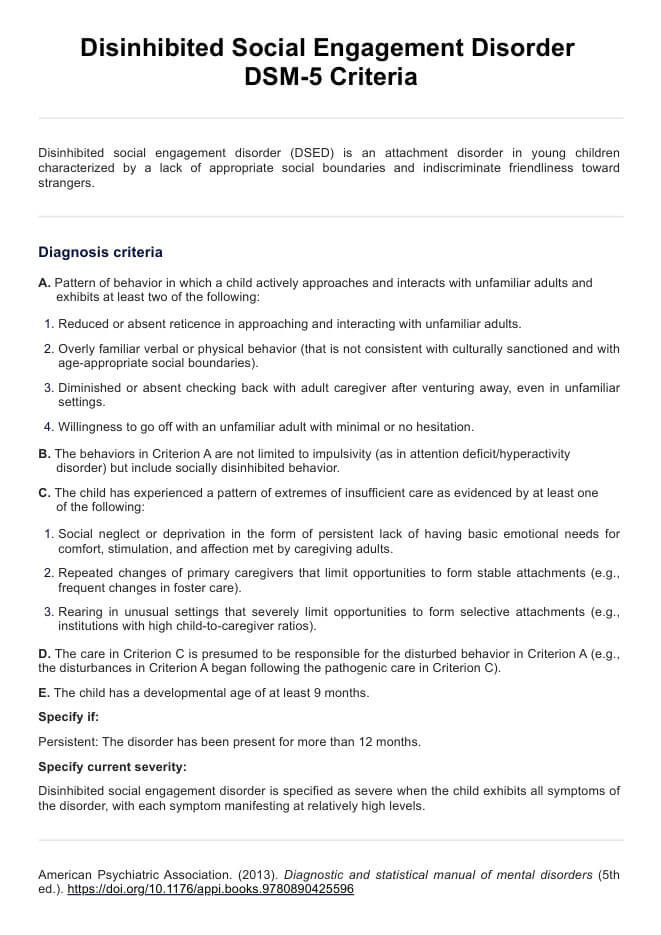
DSED is diagnosed according to specific criteria outlined in the DSM-5 (American Psychiatric Association, 2013):
A. Pattern of behavior in which a child actively approaches and interacts with unfamiliar adults and exhibits at least two of the following:
- Reduced or absent reticence in approaching and interacting with unfamiliar adults.
- 2. Overly familiar verbal or physical behavior (that is not consistent with culturally sanctioned and with age-appropriate social boundaries).
- Diminished or absent checking back with adult caregiver after venturing away, even in unfamiliar settings.
- Willingness to go off with an unfamiliar adult with minimal or no hesitation.
B. The behaviors in Criterion A are not limited to impulsivity (as in attention deficit/hyperactivity disorder) but include socially disinhibited behavior.
C. The child has experienced a pattern of extremes of insufficient care as evidenced by at least one of the following:
- Social neglect or deprivation in the form of persistent lack of having basic emotional needs for comfort, stimulation, and affection met by caregiving adults.
- Repeated changes of primary caregivers that limit opportunities to form stable attachments (e.g., frequent changes in foster care).
- Rearing in unusual settings that severely limit opportunities to form selective attachments (e.g., institutions with high child-to-caregiver ratios).
D. The care in Criterion C is presumed to be responsible for the disturbed behavior in Criterion A (e.g., the disturbances in Criterion A began following the pathogenic care in Criterion C).
E. The child has a developmental age of at least 9 months.
Specify if:
- Persistent: The disorder has been present for more than 12 months.
Specify current severity:
- Disinhibited social engagement disorder is specified as severe when the child exhibits all symptoms of the disorder, with each symptom manifesting at relatively high levels.
Differences between the DSM-4 and DSM-5 criteria
In DSM-IV, reactive attachment disorder was classified as one disorder with two subtypes, including one about indiscriminately social/disinhibited. In DSM-5, these two subtypes have been redefined as separate disorders, reactive attachment disorder and disinhibited social engagement disorder (American Psychiatric Association. (2013a). This change reflects a better understanding of the distinct characteristics and needs of children who experience social neglect or other situations that limit their ability to form attachments.
How is disinhibited social engagement disorder treated?
DSED often associated with reactive attachment disorder (RAD), is typically treated through a combination of therapeutic interventions aimed at addressing underlying attachment disorders and improving social behaviors. Key treatments include:
- Attachment-based therapy: This focuses on establishing secure attachments between the child and caregivers, often involving structured interactions to enhance trust and emotional bonding.
- Trauma-focused therapy: Addressing past neglect or trauma through specialized techniques helps mitigate the impact on social behaviors and emotional regulation, particularly important in cases where RAD coexists with DSED.
- Play therapy: Utilizing play to explore emotions and social interactions in a safe environment, promoting healthier ways of relating to others, which can be effective for children with RAD who struggle with forming attachments.
- Behavioral interventions: Implementing strategies to modify specific behaviors such as overly familiar interactions with strangers, promoting appropriate boundaries, crucial in managing both RAD and DSED symptoms.
- Family therapy: Involving caregivers to improve parenting skills, enhance understanding of the disorder, and provide consistent support, pivotal for addressing the disrupted attachment patterns seen in RAD and DSED.
- Psychiatric medications: Sometimes prescribed to manage associated symptoms like anxiety or hyperactivity, though not a primary treatment, they may support overall therapeutic efforts, especially in cases where RAD's severe emotional dysregulation impacts treatment.
Early intervention is crucial, as it can mitigate long-term effects on relationships and emotional well-being. (American Psychiatric Association, 2013).
References
American Psychiatric Association. (2013a). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association. (2013b). Highlights of changes from DSM-IV-TR to DSM-5. https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM_Changes_from_DSM-IV-TR_-to_DSM-5.pdf
Commonly asked questions
DSED is primarily caused by a history of severe social neglect or disruptions in early caregiving experiences. Factors such as frequent changes in caregivers or institutional rearing can contribute to the development of this disorder.
DSED and RAD both stem from early social neglect, but they manifest differently. RAD is characterized by inhibited, withdrawn behavior towards caregivers, while DSED involves indiscriminate, overly friendly behavior towards strangers.
According to the DSM-5, the criteria for DSED include a pattern of approaching and interacting with unfamiliar adults, exhibiting at least two of: reduced reticence, overly familiar behavior, lack of checking back with caregivers, and willingness to go off with strangers.
Related Templates

Popular Templates


-template.jpg)