Case Notes Template
Create polished case notes for your social work clients using our free Case Notes Template.

Fact Checked by RJ Gumban.


What are case notes?
Case notes are detailed records of interactions between healthcare practitioners and their clients. They serve as a comprehensive documentation of client assessments, interventions, and progress throughout the course of treatment. These notes are essential for healthcare professionals, providing a clear and concise account of each client encounter.
At their core, case notes capture key information such as the client's presenting concerns, observations made during sessions, interventions provided, and plans for future care. They typically include details about the client's appearance, behavior, mental state, and any significant events during the interaction.
While case notes are utilized across various healthcare disciplines, they are significant in social work practice. Case notes for social workers have unique characteristics reflecting the profession's holistic approach to client care.
Case Notes Template
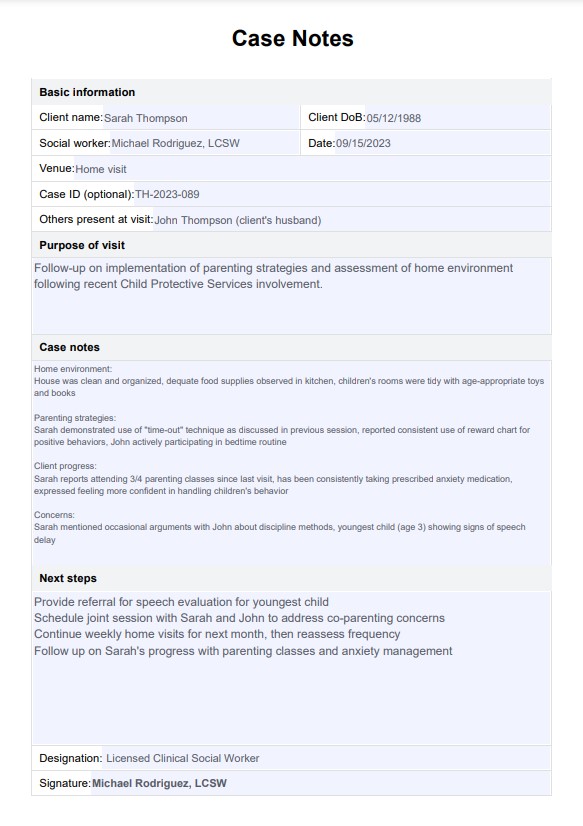
Case Notes Template Example
What are social work case notes?
Social work case notes are specialized accurate records that document interactions, assessments, and interventions with clients in the social work field.
Social work case notes typically include:
- Biopsychosocial assessments: Comprehensive evaluations of a client's biological, psychological, and social factors influencing their well-being and functioning.
- Environmental factors: Information about the client's living situation, community resources, and social support systems.
- Strengths-based observations: Identification of client strengths, resilience factors, and coping mechanisms.
- Systems interactions: Document the client's interactions with various systems, such as family, education, healthcare, or legal institutions.
- Cultural considerations: Notes on cultural factors that may impact the client's situation or treatment.
- Advocacy efforts: Records of any advocacy work done on behalf of the client.
- Referrals and collaborations: Information about referrals made to other services or collaborations with other professionals.
These notes are crucial for maintaining continuity of care, especially in settings where multiple social workers may be involved in a client's case over time. They also serve as a reflection and critical thinking tool, allowing a licensed clinical social worker to analyze patterns, identify areas for intervention, and track progress toward treatment goals.
How to use our Case Notes Template
Our Case Note Templates are designed to streamline case note recording while ensuring comprehensive and professional record-keeping.
Step 1: Gather information
Begin by collecting all relevant background information from the client interaction immediately after the session. This includes the client's presenting concerns, observations of their appearance and behavior, significant statements, interventions provided, and any plans or next steps discussed. You must also include your name as the social worker involved.
Step 2: Fill in the template fields
Proceed to complete each section of this Case Note Template with clear, concise, and objective information. You can use the case notes examples for support workers previewed on this page as you fill out the template.
Step 3: Review and refine
After completing the template, carefully review the entire note. Check for accuracy of all information, ensuring it's correct and factual. Verify that all included details are relevant to the client's care. Ensure the note is clear and easily understandable by other professionals. Confirm that all necessary information has been included.
Step 4: Secure and store
Finally, proper procedures must be followed to store the completed note securely. Electronic notes should be saved in the designated secure system, and physical copies should be filed in the appropriate location. Ensure all storage methods comply with confidentiality regulations and organizational policies.
Best practices in writing case notes
Effective case note-taking is a crucial skill for healthcare practitioners. By following best practices, it's possible to create comprehensive, accurate, and useful records that support quality care and meet legal and ethical standards.
Maintain objectivity
When recording factual case notes, prioritize objective information over subjective opinions. While professional opinions are valuable, your own subjective lens should be clearly distinguished from objective observations.
Ensure timeliness
Write case notes as soon as possible after each client interaction, especially for the initial visit. This practice ensures accuracy and completeness in documentation.
Review previous case notes
Before each session, review previous case notes to maintain continuity of care and track progress. This habit aids in updating the treatment plan and identifying new risks or concerns. You can also refer to sample case notes to serve as a guide to help you write good case notes.
Include client perspective
Document the client's concerns and response to interventions or discussions. Recording case notes with this approach demonstrates respect for service users and provides valuable context for future interactions.
Use templates carefully
Use Case Notes Templates or case management software to ensure consistency and completeness. However, be cautious not to let these tools or possible case note examples limit the individualization of each client's record.
Use professional language
Write clearly and professionally, making yourself understandable to other healthcare practitioners. Avoid jargon or colloquialisms that might be misinterpreted.
Benefits of using a Case Notes Template
A well-designed Case Notes Template can be valuable for healthcare practitioners, particularly social workers, who often deal with complex and sensitive cases. The following are numerous benefits of using this structured approach to case documentation:
Standardization and consistency
Implementing a Case Notes Template promotes uniformity across an organization. This consistency ensures that all practitioners document similar information for each client, facilitating easier case reviews and smoother information transfers between providers.
Time efficiency
A thoughtfully designed template can significantly reduce time spent on paperwork. By providing a clear structure, practitioners can focus on recording essential information without getting sidetracked or deliberating over what to include.
Legal and ethical protection
Well-structured case notes can provide legal protection for the practitioner and the organization. In the event of an audit or legal inquiry, comprehensive and consistently formatted notes demonstrate professionalism and adherence to best practices. This is especially important for social workers who often navigate sensitive situations with significant legal implications.
Commonly asked questions
To write an effective case note, use clear, objective language to document the client's current status, progress, and any significant events or interventions during the session. Structure the note chronologically, including the session's date, time, and duration. Avoid jargon or abbreviations, and ensure the note is legible and well-organized.
Case notes should be detailed enough to provide a comprehensive record of the client's treatment and progress but concise enough to be easily readable. They should include relevant details about the client's mental status, behavior, and responses to interventions, as well as any new information or insights gained during the session.
Essential information that must be included in case notes includes the client's name, date of birth, and any relevant identifying information. The note should also include the date, time, and duration of the session and the name and credentials of the clinician writing the note. Additionally, the note should document the client's presenting problem, any relevant history, the treatment plan, and any specific interventions or recommendations made during the session.
Related Templates

Popular Templates

-template.jpg)